
Abstract
Introduction: The aim of the study is to analyze the voice changes occurring during a hemodialysis session objectively and to investigate the statistical correlation between voice changes and ultrafiltration, blood pressure, dry weight and the other variables of the patients. Materials and methods: A total of 169 patients were included in the study. Electronic voice recordings of the patients were performed with the aim of making objective voice analysis before and after dialysis. Fundamental frequency measurements occurring at the level of the larynx (Fo) and harmonic-to-noise ratio (HNR) were measured from these voice recordings. Results: When the voice recordings obtained from 169 hemodialysis patients before and after dialysis were investigated, it was observed that a significant increase occurred in the Fo (from 164.52 ± 43.36 Hz to 193.19 ± 47.08 Hz, p < 0.01). When the change in HNR was investigated, a significant reduction was determined in the post-dialysis measurements (4.6 ± 3.23 dB) compared to the pre-dialysis measurements (16.10 ± 4.06 dB, p < 0.01). Mean 2.49 ± 0.83 L of ultrafiltration was performed and a significant reduction was observed in post-session body weights of the patients (p < 0.01). There was a highly statistical significance between the measurements of post-dialysis Fo and post-dialysis body weights. A highly significant correlation was determined between the amount of ultrafiltration performed and a significant increase observed in Fo before and after dialysis. Also a significant correlation was determined between the reduction in the mean post-session blood pressures and the reduction in the HNRs. Conclusion: Objective voice analysis is suggesting that it can be a simple and applicable method that can be used to determine the dry weight.
Introduction
Even though they are temporary problems related to voice experienced during or after dialysis session by the hemodialysis patients may affect them considerably and may impair their communications and quality of lives. Reduction in the quality of voice, hoarseness being in the first place, may cause severe concerns on the patients or their relatives. Since change in the voice differs considerably from patient to patient and it is expressed subjectively, it also brings along difficulties in defining and evaluating the problem. Today, it is possible to establish the voice quality and to be able to quantify the extent of dysphonia if present as clinical test with the use of voice analysis methods becoming widespread.Citation1 The aim of the study is to analyze the voice changes occurring during a hemodialysis session objectively and to investigate the correlation between the obtained variables and the other variables of the patients, ultrafiltration performed during dialysis and post-dialysis body weights being in the first place.
Materials and methods
The study was approved by the Clinical Research Ethical Committee of Istanbul Aydin University with the written document dated 19 June 2014 and numbered of 0.2.AYD.0.00.00-480/007. A total of 169 adult patients aged ≥18 years from two hemodialysis centers existing within the structure of Private Erdem Hospital who were on a chronic hemodialysis program three times a week for >6 months were included in the study. Informed consent was received from all of the patients included in the study by signing “Voluntary Informed Consent Form” which was designed for the study. Fresenius FX CorDiax High-Flux dialyzers (FX Class: 60, 80 and 100; Bad Homburg vor der Höhe, Germany) appropriate for body surface areas of all patients were used as dialyzers. Composition of the dialysate was as followings: Na = 140 mmol/L and K = 1–2 mmol/L. Arterial blood pressure measurements obtained before dialysis, during session and after session were recorded. The patients were not allowed to eat food during 4-h dialysis session. Blood samplings for blood urea nitrogen, Na and K were performed two times before dialysis and after dialysis session. The other biochemical parameters were obtained from blood samplings performed before dialysis. The amounts of ultrafiltration performed during session, body weights of the patients before and after dialysis were recorded.
The patients with acute chronic laryngitis, upper respiratory tract infections impairing voice quality, the patients with history of thyroid, parathyroid or neck surgery, the patients undergoing vocal cord surgery, thyroid dysfunction consistent with hypothyroidism or hyperthyroidism and the patients requiring parenteral nutrition were excluded from the study. Also the patients with hemodynamic impairment at a level requiring intravenous intervention during session were excluded from the study. The patients included in the study were evaluated regarding acceptance criteria by an otorhinolaryngologist before the study.
Electronic voice recordings of all of the patients were performed before and after a selected session by the same team including an otorhinolaryngologist. The voices were recorded by using Shure C606N cardioid microphone (Shure Inc., Niles, IL). Recording process was performed by holding the microphone at a distance of 10 cm and at an angle of 45° from the mouth of patient and by uttering a vowel of constant/a/for minimum 5 s. Praat software (version 4.2.17, Phonetic Sciences, University of Amsterdam) was used for voice analysis.Citation1 Harmonic-to-noise ratio (HNR) which was the ratio of the total energy of the harmonics of frequency measurements of the primitive voice occurring at the level of the larynx and the fundamental voice (Fo) and its coefficients to the energy of noise was measured for each patient before and after dialysis by the same otorhinolaryngologist.
Statistical evaluations
NCSS (Number Cruncher Statistical System) 2007 and PASS (Power Analysis and Sample Size) 2008 Statistical Software (NCSS LLC, Kaysville, UT) program was used for the statistical analysis. During the evaluation of the study data, paired samples t-test was used regarding the comparisons of descriptive statistical methods (mean, standard deviation, median, frequency and ratio) as well as comparisons of the parameters with normal distribution before and after dialysis. Pearson’s and Spearman’s correlation analysis were used to evaluate the correlations between the variables. Significance was evaluated at the lowest level of p < 0.05.
Results
A total of 169 chronic hemodialysis patients (male = 82, female = 87) with mean age of 65.06 ± 11.73 years (range: 26–90 years) from two hemodialysis centers were included in the study. The patients were on a chronic hemodialysis program for a mean period of 59.28 ± 45.90 months and their Kt/V was 1.57 ± 0.25.
General characteristics of the patients were summarized in . When the pre-dialysis and post-dialysis objective voice analysis of the patients were investigated, it was observed that a statistically significant increase occurred in the fundamental frequency measurements (Fo) occurring at the level of the larynx (from 164.52 ± 43.36 Hz to 193.19 ± 47.08 Hz; p < 0.01). When the change in HNR which was found with the ratio of the total energy of the harmonics of fundamental frequency and its coefficients to the energy of noise was investigated, a significant reduction was determined in the measurements after dialysis (4.61 ± 3.23 dB) compared to the pre-dialysis measurements (16.10 ± 4.06 dB) (p < 0.01).
Table 1. General characteristics of patients.
A mean of 2.49 ± 0.83 L ultrafiltration was performed in the patients during the dialysis and a statistically significant reduction was observed in post-dialysis body weights of the patients (71.44 ± 15.77 kg) compared to pre-dialysis body weights of the patients (73.94 ± 15.98 kg) (p < 0.01). Mean pre-dialysis systolic blood pressure, mean pre-dialysis diastolic blood pressure and mean pre-dialysis arterial pressure were 132.43 ± 17.30 mmHg, 77.10 ± 9.66 mmHg and 95.54 ± 11.41, respectively. Mean post-dialysis blood pressure measurements were 113.20 ± 18.57 mmHg, 68.05 ± 11.82 mmHg and 83.10 ± 13.34, respectively. Change between each of mean blood pressures obtained before and after dialysis was found to be statistically significant (p < 0.01). Correlations between pre-dialysis and post-dialysis data were summarized in .
Table 2. The correlation between pre-dialysis and post-dialysis parameters of the patients.
When the change between pre-dialysis and post-dialysis electrolyte levels of the patients was investigated, while there was no significance in sodium changes, as it was expected a statistically significant reduction was observed in potassium levels after dialysis (p < 0.01) Percentage rates of change in all of the measurements were summarized in .
Table 3. Rate of change of the changes observed during the session.
While there was a nearly significant correlation between mean pre-dialysis body weights (73.94 ± 15.98 kg) and pre-dialysis voice frequencies (input Fo) of the patients (p = 0.059), it was determined that there was a highly statistically significant correlation between mean post-dialysis body weights (71.44 ± 15.77 kg) and post-dialysis voice frequencies (output Fo) of the patients (, p < 0.01). When the correlation between ultrafiltration causing significant reduction in post-dialysis body weights and blood pressures observed a statistically significant reduction and voice parameters obtained from pre-dialysis and post-dialysis analysis was investigated, it was determined that:
Ultrafiltration caused statistically significant reduction in systolic, diastolic and mean blood pressures (p < 0.01) (),
Change in ultrafiltration and Fo showed a statistically significant correlation (p < 0.01) () and
Reduction in diastolic and mean arterial pressure observed during dialysis had a statistically significant correlation with the reduction in HNR (p < 0.05) ().
Table 4. The correlation of Fo with pre-dialysis and post-dialysis parameters.
Discussion
Transmission of voice in an environment depends on the features of voice and environment. One of the fundamental features of the voice is frequency and it equals to number of vibrations of the vocal folds per second. Fo means the frequency of fundamental voice occurring at the level of the larynx. Mean Fo value during normal speech is between 100–180 Hz in the males and 180–250 Hz in the females. HNR is the ratio of total energy of the fundamental voice and its harmonic components to the energy of the noise. The dB is the unit used to measure and higher values show that the ratio of noise is high in the voice.
Figure 1. Correlation between weight changes and blood pressure changes of the patients.
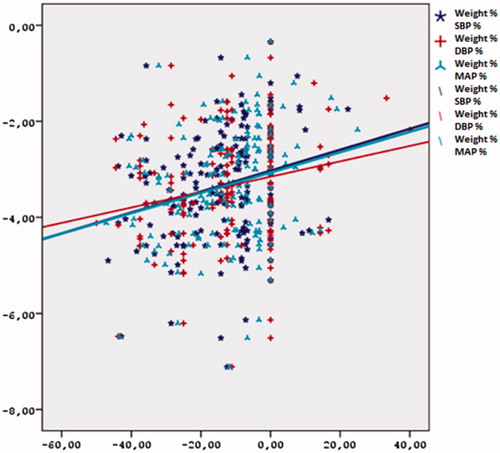
Figure 2. Correlation between changes in Fo and the amount of ultrafiltration.
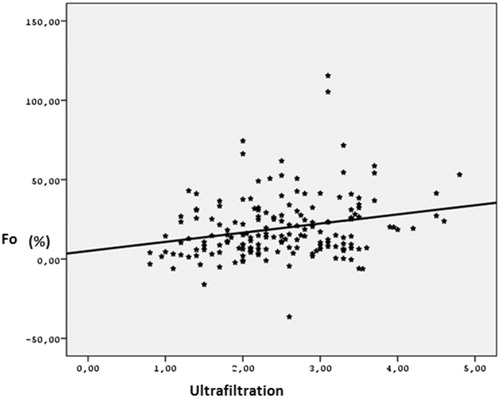
Table 5. The correlation between ultrafiltration performed during dialysis and blood pressure changes and voice changes.
Identification of voice problems and investigation of pathophysiology became the most important field of occupation of otorhinolaryngology.Citation2,Citation3 Impairments observed in the voice quality of hemodialysis patients can be an important source of anxiety for the patients and their relatives. Notwithstanding, there are quite limited number of studies performed on voice changes in the patients with renal failure and dialysis patients. At the beginning, the thought of reduction in the quality of voice observed in the dialysis patients occurred with the effect of stress was adopted.Citation4 However, in the following years, the thought of impairment in the voice was associated with extracellular volume reduction came to the forefront. Fisher et al.Citation5 reported that ultrafiltration caused voice symptoms in six dialysis patients.
The importance of hydration has been established in vocal cord physiology and adequate hydration of vocal cords and the whole body is essential for phonation.Citation6 Nonetheless, usually there is a constant hypervolemic state in hemodialysis patients but it can be controlled only with ultrafiltration performed during the session. In our study, mean amount of ultrafiltration performed in the patients was 2.49 ± 0.83 L and the difference between pre-dialysis and post-dialysis body weights (−3.33 ± 1.17%) was found to be statistically significant (p < 0.01). There are many studies investigating the volume state in dialysis patients performed on “dry weight” defined to be the lowest weight hemodynamically is tolerated after dialysis and hypervolemic state of the patient is prevented.Citation7–9 Hemodynamic changes accompanying to the ultrafiltration performed to prevent hypervolemia are also among well-studied subjects.Citation10–13 Also in our study, with a mean amount of ultrafiltration of 2.49 ± 0.83 L performed, significant reduction was observed in post-dialysis systolic blood pressure, diastolic blood pressure and mean arterial blood pressure (113.20 ± 18.57 mmHg, 68.05 ± 11.82 mmHg, 83.10 ± 13.34, respectively) compared to pre-dialysis systolic blood pressure, diastolic blood pressure and mean arterial blood pressure (132.43 ± 17.30 mmHg, 77.10 ± 9.66 mmHg and 95.54 ± 11.41, respectively). Namely, there is a negative significant correlation between ultrafiltration and blood pressure measurements (p < 0.01).
In the study performed by ZumrutdalCitation14 and evaluating the voice in dialysis patients subjectively, it was emphasized that hoarseness was an overlooked complication (15.2%) of hemodialysis. In the study conducted by Ori et al.Citation15 to evaluate the effect of hemodialysis on the thickness of vocal fold, endoscopic nasopharyngolaryngoscopy was performed before and after hemodialysis in 25 chronic hemodialysis patients and vocal fold thickening was observed in 72% of the patients. The correlation between this thickening and interdialytic weight loss and reduction in blood pressure was found to be significant. The result was associated with volume loss.
Kumar and BhatCitation16 performed objective voice analysis and reported that significant voice changes were present in the patients with chronic renal failure compared to the healthy control group. Balasubramanium and BhatCitation17 compared 30 dialysis patients with 60 healthy adults and they found that the Fo levels to be significantly higher in dialysis patients.
There are a few study performed with lower number of patients evaluating the voice changes in the session objectively and investigating its correlation with ultrafiltration and hemodynamic changes.Citation18,Citation19 These studies were designed and published by otorhinolaryngologists. In objective voice analysis performed by Hamdan et al.Citation18 in 57 hemodialysis patients before and after dialysis, it was reported that a significant increase occurred in habitual frequency levels of voice after dialysis, but significance between the voice and patient characteristics and hemodialysis variables were not investigated.
In the study performed by Jung et al.Citation19 investigating objective voice data of 55 hemodialysis patients before and after dialysis, the authors reported that a significant increase occurred in the Fo of all patients. But the authors reported that there was no correlation between weight changes and acoustic parameters of the patients. Also in our study, when the voice recordings of patients before and after dialysis were investigated objectively, it was observed that a statistically significant increase occurred in the Fo. Additionally, when the change in the HNRs was investigated, a statistically significant reduction was determined after dialysis compared to pre-dialysis ratios (p < 0.01).
In our study designed to investigate the importance of voice measurements in dialysis practice; the effects of ultrafiltration and blood pressure changes recorded during dialysis on the voice parameters were evaluated and apart from the other studies, the relationships of voice parameters of all patients with pre-dialysis and post-dialysis weights and correlation of change in the voice observed objectively during dialysis and change in blood pressures were investigated.
Conclusion
The Fo increased significantly after dialysis compared to pre-dialysis measurements. While there is a nearly statistically significant correlation between pre-dialysis Fo and pre-dialysis weights, there is a high statistical significance between post-dialysis Fo and post-dialysis weights of the patients. There is a high significant correlation between significant increase observed in Fo during dialysis session and amount of ultrafiltration performed and reduction in post-session blood pressures. The results are suggesting that the change in fundamental frequency obtained by objective analysis of the voice during dialysis session is highly correlated with volume and hemodynamic changes in the patients and it can be a simple and applicable method that can be used to determine the dry weight.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Núñez Batalla F, González Márquez R, Peláez González MB, González Laborda I, Fernández Fernández M, Morato Galán M. Acoustic voice analysis using the Praat program: Comparative study with the Dr. Speech program. Acta Otorrinolaringol Esp. 2014;65(3):170–176
- Aithal VU, Bellur R, John S, Varghese C, Guddattu V. Acoustic analysis of voice in normal and high pitch phonation: A comparative study. Folia Phoniatr Logop. 2012;64(1):48–53
- Eysholdt U. Hoarseness: Biomechanisms and quantitative laryngoscopy. HNO. 2014;62(7):541–552
- Nesić M, Veljković S, Obrenović J, Cekić S, Velicković D, Radenković M. Voice frequencies in patients treated with chronic hemodialysis. Srp Arh Celok Lek. 1996;124(Suppl. 1):99–101
- Fisher KV, Ligon J, Sobecks JL, Roxe DM. Phonatory effects of body fluid removal. J Speech Lang Hear Res. 2001;44(2):354–367
- Sivasankar M, Leydon C. The role of hydration in vocal fold physiology. Curr Opin Otolaryngol Head Neck Surg. 2010;18(3):171–175
- Leunissen KML. Fluid status in hemodialysed patients. Nephrol Dial Transplant. 1995;10:153–155
- Charra B. ‘Dry weight’ in dialysis: The history of a concept. Nephrol Dial Transplant. 1998;13:1882–1885
- Charra B, Laurent G, Chazot C, et al. Clinical assessment of dry weight. Nephrol Dial Transplant. 1996;11(Suppl. 2):16–19
- Luik AJ, Charra B, Katzarski K, et al. Blood pressure control and hemodynamic changes in patients on long time dialysis treatment. Blood Purif. 1998;16:197–209
- Wizemann V, Schilling M. Dilemma of assessing volume state: The use and limitations of a clinical score. Nephrol Dial Transplant. 1995;10:2114–2117
- Sandberg F, Bailón R, Hernando D, et al. Prediction of hypotension in hemodialysis patients. Physiol Meas. 2014;35(9):1885–1898
- Weiner DE, Brunelli SM, Hunt A, et al. Improving clinical outcomes among hemodialysis patients: Proposal for a “volume first” approach from the chief medical officers of US dialysis providers. Am J Kidney Dis. 2014;64(5):685–695
- Zumrutdal A. An overlooked complication of hemodialysis: Hoarseness. Hemodial Int. 2013;17(4):633–638
- Ori Y, Sabo R, Binder Y, et al. Effect of hemodialysis on the thickness of vocal folds: A possible explanation for postdialysis hoarseness. Nephron Clin Pract. 2006;103(4):c144–c148
- Kumar RB, Bhat JS. Voice in chronic renal failure. J Voice. 2010;24(6):690–693
- Balasubramanium RK, Bhat JS. Voice in chronic hemodialyzed individuals. Indian J Med Sci. 2010;64(2):66–71
- Hamdan AL, Medawar W, Younes A, Bikhazi H, Fuleihan N. The effect of hemodialysis on voice: An acoustic analysis. J Voice. 2005;19(2):290–295
- Jung SY, Ryu JH, Park HS, Chung SM, Ryu DR, Kim HS. Voice change in end-stage renal disease patients after hemodialysis: Correlation of subjective hoarseness and objective acoustic parameters. J Voice. 2014;28(2):226–230