
Abstract
Aims: Anemia and vitamin D deficiency (VDD) are both very important health issues, recent accumulating evidence shows that VDD is prevalent in individuals with anemia. This meta-analysis aimed to detect a relationship between VDD and anemia. Methods: We identified eligible studies by searching the Pub Med, Embase and Cochrane Library before October 2014. Quality assessments were performed with the Newcastle–Ottawa Scale. Heterogeneity was evaluated by Cochran’s Q test and source of heterogeneity was detected by subgroup analysis and sensitivity analysis. Results: A total of seven studies involving 5183 participants were included in the meta-analysis. VDD was associated with an increased incidence of anemia (OR = 2.25, 95% CI = 1.47–3.44), with significant evidence of heterogeneity among these studies (p for heterogeneity <0.001, I2 = 84.0%). The subgroup and sensitivity analysis confirmed the stability of the results and no publication bias was detected. Conclusion: Our outcomes showed that VDD increased the risk of developing anemia. More researches are warranted to clarify an understanding of the association between VDD and risk of anemia.
Introduction
Anemia is a major global health concern due to its high prevalence and association with substantial morbidity and mortality.Citation1,Citation2 The World Health Organization (WHO) estimates that about 2 billion people in the world are suffering from this disease, and that approximately 50% of all anemia cases are diagnosed as iron deficiency anemia (IDA).Citation3,Citation4 It is known that a variety of causes, such as inadequate iron intake, chronic blood loss, chronic disease, malabsorption, hemolysis or a combination of these, can induce anemia.Citation5–7 Consequently, efforts to identify less well-known, but potentially modifiable, factors associated with anemia will be required to reduce the large burden of anemia.
Vitamin D deficiency (VDD) is also an important issue in public heath because it is associated with a wide range of illnesses and chronic conditions, such as osteoporosis, cancer and metabolic syndrome.Citation8 In addition, not only VDD but also alterations of vitamin D signaling are also implicated especially in patients with renal diseases.Citation9 Vitamin D requirements are fulfilled by ingestion of food or by skin exposure to ultraviolet light for a sufficient period of time. In recent years, an increasing body of evidence indicates that VDD was associated with increased risk for anemia, a common condition experienced by up to 20% of children.Citation10 However, large-scale studies had yet to demonstrate the relationship between vitamin D and hemoglobin levels in the general population. Whether VDD was an independent risk factor of anemia remains unclear. Thus, we were interested in further investigating VDD and the development of anemia and conducted here a meta-analysis of published literature to investigate an epidemiologic relationship, if any, existed between VDD and the risk of anemia.
Materials and methods
Search strategy
A systematic search of the literature published earlier than October 2014 was conducted in Pub Med, The Cochrane Library and Embase databases by two independent investigators to identify related articles. The following search terms were used: “vitamin D” or “25-hydroxy vitamin D” or “25(OH)D” or “anemia” or “anaemia”. No language and time restrictions were done. The titles and abstracts of the resulted articles were checked. Duplicate citations were then removed. After excluding nonrelated articles, full-text articles were retrieved. In addition, a manual search of references was performed to find other relevant articles.
Inclusion and exclusion criteria
Eligible articles should meet all the following criteria: (1) all available retrospective comparative studies (cohort or case-control studies) that had comparative data of the association between VDD and anemia; (2) one of the outcome interest was anemia; (3) the control group should be healthy people, and patients of the experimental group were anemia; (4) should evaluate the association between serum vitamin D levels and anemia; (5) relative risks (RRs) or odds ratio (OR) estimates and their 95% confidence intervals (95% CI) were reported or provided sufficient information to calculate them.
Studies that were excluded: (1) review articles, case reports and animal experimental studies; (2) articles about association of VDD and anemia were excluded for which VDD were included in both the case and control groups without non-VDD to compare; (3) patients with malignant tumors or the other chronic diseases, such as congestive heart failure, chronic renal failure; (4) they provided only an effect estimate with no means to calculate a CI. Any discrepancies between reviewers on inclusion of a study were resolved by a third reviewer or by consensus. Articles or reports from non-peer-reviewed sources were not included in this meta-analysis. In the event of multiple publications from the same or overlapping study populations, only the most relevant one was selected. Reviews or editorials, letters to the editor without original data and case reports were excluded.
Data extraction
Two investigators independently performed the data extraction. When discrepancies were found, a third investigator would make the definitive decision for data extraction. The extracted information included: the first author’s name, year of publication, country of origin, study design, sample size, participants’ ages, criteria for diagnosis of VDD, definition of anemia and measure of association. The quality of each study was evaluated independently by two authors who used the nine-score Newcastle–Ottawa Scale (NOS).Citation11
Statistical analysis
Fixed-effect or random-effect models were appropriately used to calculate a pooled adjusted OR with 95% CI.Citation12,Citation13 Between-study heterogeneity was assessed using Cochran’s Q test and I2 index. p > 0.05 for the Q-test indicated a lack of heterogeneity among the studies. The pooled OR estimate of each study was calculated by the fixed-effect model. Otherwise, the random-effect model was used. In case of significant between-study heterogeneity, we used subgroup analysis and meta-regression to find out possible sources of heterogeneity. Sensitivity analysis was performed by sequential omission of individual studies under various contrasts to reflect the influence of the individual data to the pooled ORs and evaluate the stability of the results. Potential publication bias was assessed by visual inspection of the Begg’s funnel plots in which the log ORs were plotted against their SEs. We also performed the Begg’s and Egger’s tests to evaluate the presence of publication bias.Citation14,Citation15 The STATA 12.0 statistical software (Stata Corporation, College Station, TX) was used for all statistical analysis. p < 0.05 was considered statistically significant.
Results
Literature search
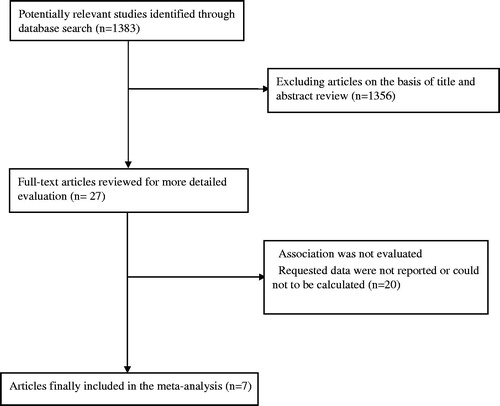
In total, 1383 articles were found in our initial search. We excluded 1356 articles through reading the title and abstract. Another 20 papers were excluded because association of interest was not evaluated, requested data were not reported, of duplicate papers of the same studies, Finally, seven studies matched the selection criteria and were suitable for our meta-analysis.Citation16–22 Three of these studies were cross-sectional, one study was a historical cohort study and three studies were case-control studies. A flow-diagram for the selection of studies to include in our meta-analysis is shown in .
Figure 1. Flow chart of study selection.
Study characteristics
The key characteristics of the included studies are provided in . Studies were published between 2010 and 2013. Two studies originated from the United StatesCitation16,Citation17 and one study from France.Citation20 The remaining four studies were from Asian countries, including: two from Korea,Citation18,Citation22 one from ChinaCitation19 and one from Bahrain.Citation21 A total of 5183 participants were included in our meta-analysis. Sample sizes ranged from 82 to 2610. For all studies in this meta-analysis, VDD was defined as serum total 25(OH)D concentration <30 ng/mL or <20 ng/mL. Anemia was defined according to WHO criteria in five studies. In the other studies, anemia was defined as a hemoglobin <11 g/dL or hemoglobin ≤11 g/dL and ferritin ≤12 ng/mL.
Table 1. Baseline characteristics of the included studies.
Main analysis
shows the results from the random-effect model combining the ORs for anemia. VDD was significantly associated with increased risk of anemia (OR = 2.25, 95% CI = 1.47–3.44) with evidence of between-study heterogeneity (I2 = 84.0%, p for heterogeneity <0.001). In a sensitivity analysis in which we removed one study at a time and analyzed the rest, the ORs ranged from 2.52 (95% CI = 1.45–4.38) after excluding the study which carried the most weightCitation17 to 2.07 (95% CI = 1.34–3.18) after excluding the study which carried the least weight.Citation22 Subgroup analysis was performed by geographical region, study design, age and VDD diagnostic criteria (). The summary estimates were significantly higher for studies conducted in Europe and in Asia than North America, and for serum vitamin D levels <20 ng/mL than for serum vitamin D levels <30 ng/mL. The summary OR was 1.87 (95% CI = 1.08–3.23) in cross-sectional studies. However, VDD was not associated with anemia incidence in case-control studies of VDD patients (OR = 3.98, 95% CI = 0.91–17.43). The positive association between VDD and anemia incidence was observed in adults (OR = 2.33, 95% CI = 1.43–3.80), but not in children (OR = 2.24, 95% CI = 0.54–9.29).
Figure 2. Forest plot showing risk estimates from our included studies estimating the association between VDD and risk for anemia.
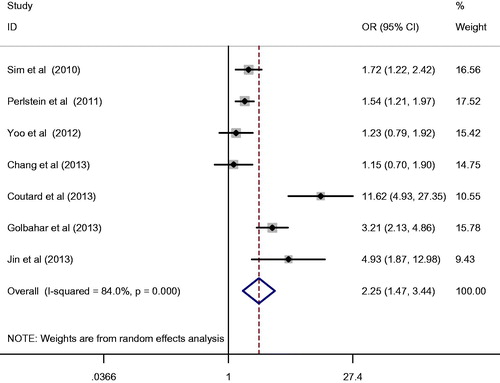
Table 2. Summary of pooled odds ratios for association between VDD and anemia.
Sensitivity analysis and publication bias
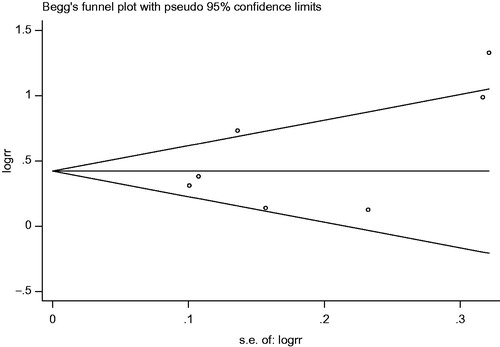
Sensitivity analysis was conducted to explore potential sources of heterogeneity in the association between VDD and anemia. After excluding one study at a time, it confirmed the significant association between VDD and anemia (). There was no evidence of publication bias on the basis of the Begg’s test (p = 0.37) and the Egger’s test (p = 0.26). Funnel plots demonstrated no visual evidence of publication bias ().
Figure 3. Results of sensitivity analysis for the current meta-analysis.
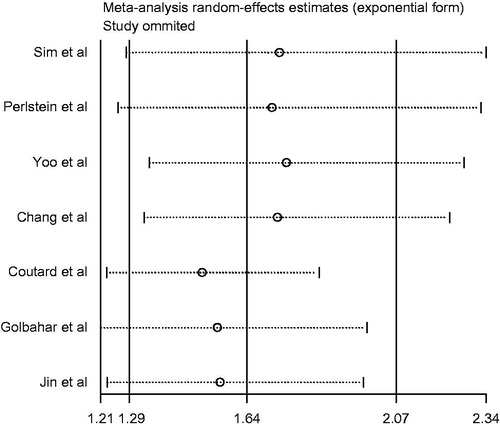
Figure 4. Begg’s funnel plot for publication bias evaluating the association between VDD and anemia.
Discussion
Anemia and VDD were both important health issues. Findings of this meta-analysis of observational studies indicated that compared with non-VDD or general population, individuals with VDD might be associated with an 64% increased risk of anemia. It tended to be more remarkable for studies with a rate ratio or hazard ratio as the measure of relative risk than for studies with a standardized incidence ratio. Our meta-analysis showed significant between-study heterogeneity, and then we carried out sensitive analysis using I2 > 50% as the criterion. After exclusion of two articleCitation16,Citation20 that was key contributors to the between-study heterogeneity, we found no significantly different OR.
Vitamin D has long been recognized for its role in regulating calcium, phosphorus and bone metabolism, but in recent years it has received attention as a regulator of a variety of biological functions, including immune function, cellular proliferation and cardiovascular function.Citation23–25 Vitamin D plays an important role on the pathogenesis of anemia. Nowadays, a new guideline of the American Academy of pediatrics is that all infants, children and adolescents have a minimum daily intake of 400 IU of vitamin D beginning soon after birth and this replaces the previous recommendation of a minimum daily intake of 200 IU of vitamin D supplementation beginning in the first 2 months after birth and continuing through adolescence.Citation26
The underlying mechanisms involved in the association between VDD and anemia have evoked a huge interest from nutritionists, scientists, clinicians and the public. The exact mechanism of association of VDD with anemia is still not known. Vitamin D is reported to stimulate erythroid precursors and vitamin D receptors have been discovered in numerous non-renal target tissues including the bone marrow.Citation27,Citation28 Vitamin D and its metabolites are present in many tissues, as are the receptors for the active form of vitamin D, calcitriol. Calcitriol plays a key role in the regulation of immune function by inhibiting the expression of proinflammatory cytokines by a variety of immune cells, thus providing negative feedback to prevent excessive inflammatory.Citation23 In vivo and in vitro studies have demonstrated that calcitriol reduces cytokine production leading to the reduction of inflammatory milieu and anemia.Citation29
There is another explanation. VDD may stimulate immune cells within the bone marrow micro-environment to produce cytokines, inducing impaired erythropoiesis.Citation30 Vitamin D therapy can improve altered iron homeostasis associated with anemia of chronic kidney disease in VDD patients. Furthermore, high-dose vitamin D therapy impacts systemic hepcidin levels in subjects with early stage chronic kidney disease. Vitamin D regulates the hepcidin–ferroportin axis in macrophages which may facilitate iron utilization.Citation31 Based on these, further mechanism researches need to be conducted to evaluate whether these is a direct causal effect of VDD on anemia.
These are several limitations that need to be taken into account when considering its results in our meta-analysis. First, there was substantial heterogeneity in our studies. We therefore used random-effects models to account for both within- and between-study variability. The sensitivity analysis that was performed did not materially change the results, increasing the confidence that can be placed in these results when applying the conclusion in practice. Second, one potential limitation of the present meta-analysis was the various methods of assessment for VDD and anemia used among studies. However, the results did not significantly change after the exclusion of two studiesCitation16,Citation21 that the serum vitamin D levels <30 ng/mL.
In conclusion, results of this meta-analysis suggest a potential hazardous effect of VDD for developing anemia. The present findings may have potentially broad public health implications given the high prevalence of VDD in some countries. Additionally, further clinical and experimental studies may be warranted to validate the present findings and determine whether the correction of VDD can ameliorate anemia.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Anand I, McMurray JJ, Whitmore J, et al. Anemia and its relationship to clinical outcome in heart failure. Circulation. 2004;110:149–154
- Zakai NA, Katz R, Hirsch C, et al. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: The Cardiovascular Health Study. Arch Intern Med. 2005;165:2214–2220
- Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet. 2007;370:511–520
- Clark SF. Iron deficiency anemia: Diagnosis and management. Curr Opin Gastroenterol. 2009;25:122–128
- Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med. 2005;352:1011–1023
- Annibale B, Marignani M, Monarca B, et al. Reversal of iron deficiency anemia after Helicobacter pylori eradication in patients with asymptomatic gastritis. Ann Intern Med. 1999;131:668–672
- Gasche C, Lomer MC, Cavill I, Weiss G. Iron, anaemia, and inflammatory bowel diseases. Gut. 2004;53:1190–1197
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281
- Santoro D, Gagliostro G, Alibrandi A, et al. Vitamin D receptor gene polymorphism and left ventricular hypertrophy in chronic kidney disease. Nutrients. 2014;6:1029–1037
- Polhamus B, Dalenius K, Thompson D, et al. Pediatric nutrition surveillance. Nutr Clin Care. 2003;6:132–134
- Stang A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–605
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–748
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101
- Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634
- Sim JJ, Lac PT, Liu IL, et al. Vitamin D deficiency and anemia: A cross-sectional study. Ann Hematol. 2010;89:447–452
- Perlstein TS, Pande R, Berliner N, Vanasse GJ. Prevalence of 25-hydroxyvitamin D deficiency in subgroups of elderly persons with anemia: Association with anemia of inflammation. Blood. 2011;117:2800–2806
- Yoo EH, Cho HJ. Prevalence of 25-hydroxyvitamin D deficiency in Korean patients with anemia. Blood. 2012;120:21
- Chang L, Liu X, Shi H, Dai W, Wang H, Jiang Y. Association of 25-hydroxyvitamin D with Hb and lead in children: A Chinese population-based study. Public Health Nutr. 2014;17: 827–832
- Coutard A, Garlantezec R, Estivin S, Andro M, Gentric A. Association of vitamin D deficiency and anemia in a hospitalized geriatric population: Denutrition as a confounding factor. Ann Hematol. 2013;92:615–619
- Golbahar J, Altayab D, Carreon E, Darwish A. Association of vitamin D deficiency and hyperparathyroidism with anemia: A cross-sectional study. J Blood Med. 2013;4:123–128
- Jin HJ, Lee JH, Kim MK. The prevalence of vitamin D deficiency in iron-deficient and normal children under the age of 24 months. Blood Res. 2013;48:40–45
- Bikle D. Nonclassic actions of vitamin D. J Clin Endocrinol Metab. 2009;94:26–34
- Baeke F, Gysemans C, Korf H, Mathieu C. Vitamin D insufficiency: Implications for the immune system. Pediatr Nephrol. 2010;25:1597–1606
- Adams JS, Hewison M. Unexpected actions of vitamin D: New perspectives on the regulation of innate and adaptive immunity. Nat Clin Pract Endocrinol Metab. 2008;4:80–90
- Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142–1152
- Reichel H, Koeffler HP, Norman AW. The role of the vitamin D endocrine system in health and disease. N Engl J Med. 1989;320:980–991
- Norman AW. Minireview: Vitamin D receptor: New assignments for an already busy receptor. Endocrinology. 2006;147:5542–5548
- Blazsek I, Farabos C, Quittet P, et al. Bone marrow stromal cell defects and 1 alpha,25-dihydroxyvitamin D3 deficiency underlying human myeloid leukemias. Cancer Detect Prev. 1996;20:31–42
- Icardi A, Paoletti E, De Nicola L, Mazzaferro S, Russo R, Cozzolino M. Renal anaemia and EPO hyporesponsiveness associated with vitamin D deficiency: The potential role of inflammation. Nephrol Dial Transplant. 2013;28:1672–1679
- Zughaier SM, Alvarez JA, Sloan JH, Konrad RJ, Tangpricha V. The role of vitamin D in regulating the iron–hepcidin–ferroportin axis in monocytes. J Clin Transl Endocrinol. 2014;1:19–25