Abstract
Purpose: To report a case of cytomegalovirus (CMV) retinitis in an HIV-negative, iatrogenically immunosuppressed patient with chronic uveitis following intravitreal triamcinolone acetonide (IVTA).
Design: Observational case report. Methods: A 56-year-old female with chronic idiopathic panuveitis on azathioprine received a single 4-mg IVTA injection for macular edema and presented after 6 months with severe retinitis.
Results: CMV was confirmed by polymerase chain reaction of vitreous fluid. The retinitis responded well to intravitreal ganciclovir, but she developed a rhegmatogenous retinal detachment and underwent vitrectomy with silicone oil tamponade.
Conclusions: Sight-threatening CMV retinitis may develop in HIV-negative, immunosuppressed individuals after IVTA. Regular fundoscopy for up to 9 months after IVTA is recommended.
CMV retinitis is a well-known complication of HIV and AIDS, which typically occurs when the CD4 cell count falls below 50. It may occur in HIV-negative patients who are on systemic immunosuppression. Recent reports have emerged of CMVR following intravitreal injections of TA in HIV-negative patients.Citation1–5 We describe a case of CMVR in an HIV-negative patient on long-term azathioprine therapy for unilateral, chronic, idiopathic panuveitis who developed severe sight-threatening CMVR following a single 4-mg intravitreal injection of TA.
Case Report
A 56-year-old female with a 4-year history of chronic, idiopathic, noninfectious panuveitis of the left eye was treated with systemic azathioprine 100 mg daily (2 mg/kg) for 2 years. After her uveitis became quiescent she underwent cataract surgery with a primary lens implant in October 2010. Postoperatively her uveitis remained well controlled with additional topical and high-dose oral corticosteroids. However, 8 weeks postoperatively she presented with a reduced visual acuity of 20/200 due to macular edema, which did not resolve with steroid and nonsteroidal anti-inflammatory drops.
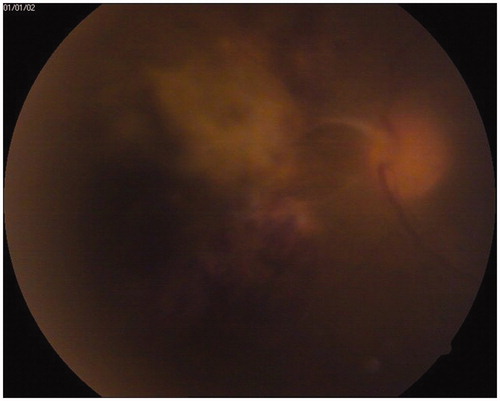
A single 4-mg IVTA injection was administered in February 2011, resulting in a significant reduction in macular edema and an improvement in visual acuity to 20/60. Her uveitis remained well controlled on azathioprine 100 mg daily, topical corticosteroids, and 10 mg prednisolone orally with a trace of persistent vitreous and anterior chamber inflammation. In August 2011, 6 months after the IVTA injection, she presented with an acute loss of temporal visual field due to extensive retinal necrosis involving the nasal and inferior retina (). She had count fingers visual acuity due to visually significant vitreous haze. There was no anterior segment inflammation. Polymerase chain reaction of vitreous fluid was positive for CMV DNA and serum HIV antibody testing was negative.
FIGURE 1. CMV retinitis involving the nasal retina.
The azathioprine was discontinued and 2 mg of intravitreal ganciclovir was given twice weekly by intravitreous injection for 3 weeks, resulting in a visible improvement in the retinitis. One month after the ganciclovir injections she developed an inferior rhegmatogenous retinal detachment necessitating vitrectomy with chronic silicone oil tamponade.
Discussion
CMV retinitis following intravitreal TA is a rare complication and appears to be caused by profound local immunosuppression in susceptible patients. Previously reported cases of CMV retinitis following TA have been described, mostly in elderly diabeticsCitation1–4 and once before in a 30-year-old with Behçet disease on chronic high-dose azathioprine and corticosteroids.Citation5 To our knowledge this is the second report of CMV retinitis following IVTA in a younger, HIV-negative patient on systemic immunosuppression for chronic uveitis. In our patient, the indication for IVTA was persistent macular edema following cataract surgery in a quiescent uveitic eye, while in previously reported cases there was a variety of indications, including persistent macular edema following a branch retinal vein occlusion,Citation1 diabetic macular edema,Citation2 age-related macular edema with choroidal neovascularisation,Citation3,Citation4 central retinal vein occlusion,Citation4 and severe panuveitis due to Behçet disease.Citation5
This case report highlights the potential danger of the reactivation of latent CMV in younger, iatrogenically immunosuppressed individuals receiving additional local immunosuppression through intraocular long-acting corticosteroid injections. In our patient the CMV retinitis manifested 6 months after the IVTA injection and in previously reported cases the range of presentation was 3–9 months.Citation1–5 Given that the maximum immunosuppressive effect of triamcinolone in the vitreous is around 2–3 months, it is likely that the CMV retinitis was in fact present earlier than the eventual clinical manifestation and that the vitreous haze present was a manifestation of immune recovery uveitis. This delayed manifestation of a sight-threatening complication compels clinicians to perform periodic fundoscopy for up to 9 months after the IVTA injection in these susceptible individuals.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Vertes D, Snyers B, De Potter P. Cytomegalovirus retinitis after low-dose intravitreous triamcinolone acetonide in an immunocompetent patient: a warning for the widespread use of intravitreous corticosteroids. Int Ophthalmol. 2010;30:595–597
- Saidel MA, Berreen J, Margolis TP. Cytomegalovirus retinitis after intravenous triamcinolone in an immunocompromised patient. Am J Ophthalmol. 2005;140:1141–1143
- Toyokawa N, Kimura H, Kuroda S. Cytomegalovirus retinitis after subtenon triamcinolone acetonide and intravitreal injection of anti-vascular endothelial growth factor in an immunocompetent patient with age-related macular degeneration and diabetes mellitus. Jpn J Ophthalmol. 2010;54:166–168
- Delyfer MN, Rougier MB, Hubschman JP, et al. Cytomegalovirus retinitis following intravitreal injection of triamcinolone: report of two cases. Acta Ophthalmol Scand. 2007;85:681–683
- Tugal-Tutkun I, Araz B, Cagatay A. CMV retinitis after intravitreal triamcinolone acetonide injection in a patient with Behçet’s uveitis. Int Ophthalmol. 2010;30:591–593