Abstract
Objective: It has been suggested that robotic-assisted remote telepresence surgery with a signal transmission latency of greater than 300 ms may not be possible. Methods: We evaluated the impact of four different latencies of up to 500 ms on task completion and error rate in five surgeons after completion of three different surgical tasks. Results: The surgeons were able to complete all tasks with a latency of 500 ms. However, higher latency was associated with higher error rates and task completion time (TCT). There were significant variations between surgeons and different tasks. Conclusion: Surgeons are able to complete tasks with a signal transmission latency of up to 500 ms. The clinical impact of slower TCT and increased error rates encountered at higher latency needs to be established.
Introduction
The first robotic-assisted remote telepresence surgery was performed by Professor Jacques Marescaux at the IRCAD/Hôpital Civil, Strasbourg, France on 7th September 2001 Citation[1] using the Zeus TS Surgical System (Computer Motion Inc., Goleta, CA). A dedicated asynchronous transfer mode (ATM) network was used to connect the surgical console of the Zeus TS system situated in New York City to three robotic arms at IRCAD/Hôpital Civil, the site of the laparoscopic cholecystectomy. The reported latency for this procedure was 155 ms Citation[1]. At this latency, Professor Marescaux reported no important impact on his ability to perform fine surgical movements Citation[1]. He completed the operation successfully in 54 min Citation[1]. His team had performed preliminary tests which suggested that tasks could be completed without important impact on precision at latencies of up to 300 ms. Unfortunately, the details and extent of these tests have not yet been published.
RARTS, a specialized application of telerobotic surgery, has the capability to allow a surgeon to complete surgical procedures (laparoscopic or open) on a patient located remote from the surgeon, regardless of distance. RARTS can also allow an expert surgeon to provide telerobotic assistance, enabling a distant surgeon to perform more complex laparoscopic or open procedures in rural and remote parts of the world. In the future, this technology may have important implications for the provision of high quality advanced surgical care in remote areas of the world, as well as in combat situations and in the space station where access to a surgeon is not available.
Although a dedicated ATM line is capable of providing transmission of signals at the speed of light without significant delay from point to point at a bandwidth of up to 155 Mbp or more, this technology is not widely available in remote and rural areas. Currently, the most widely available accessible modes of communication are either a satellite technology (latency of ∼500 ms) or an Internet Protocol–Virtual Private Network (IP–VPN) with variable latency. Therefore, it is essential to evaluate whether a surgical task can be completed with adequate precision at a latency approaching 500 ms. The purpose of this study was to evaluate the impact of latency on the ability to complete surgical tasks without clinically important error.
Methods
Five laparoscopic surgeons with varying degrees of robotic surgical experience were asked to complete three specific surgical tasks at latencies of 0, 175, 300, and 500 ms. Each task was graded by completion time and error rate. The order of latencies used during each task was randomized, and the surgeon was blinded to the latency at all times. Each task was completed three times at each latency. An independent observer was used to record the completion time and the number of errors.
Creation of latency
The robotic console was situated in a different room from the robotic arms, which were attached to a table and positioned around a laparoscopic trainer (). The connection between the console and the arms was either direct (for real time) or via a commercially available VPN network (Bell Canada, Toronto, ON) using two CODECS (Amnis Systems, Palo Alto, CA) to compress and decompress the video signals. NetDisturb software (ZTI Computing and Telecommunications, Lannion, France) was used to introduce fixed time delays into the network, thus allowing variation in time delay from real time to 175, 300, and 500 ms. There was minor degradation of video signals using the latency software, codecs, and VPN network (<10%).
Figure 1. Telerobotic assembly with the surgeon behind the console in a different room from the robotic arms.


The different tasks
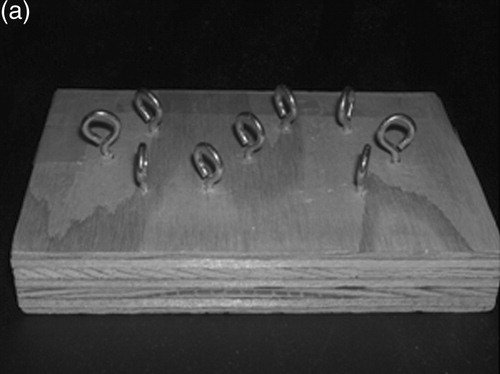
Task 1 was designed to evaluate two-handed maneuvering. The surgeons were presented with a wooden board with nine metal eyelets fastened in an ‘S’ pattern 1.5 cm apart (). This was fixed firmly inside a laparoscopic trainer. Using two robotic needle drivers and 2-0 silk (the silk was on a ski needle which was cut to remove the curved portion), the surgeons started from the lower right eyelet and passed the suture through each eyelet in the ‘S’ pattern, finally concluding at the upper left. The clock was started after the surgeon had positioned the needle in the driver and was stopped when it was extracted from the last eyelet. An error was recorded each time, the surgeon failed to pass the needle through an eyelet, dropped the needle while passing through the eyelet, or failed to pass the needle from one hand to the other while passing through the eyelet.
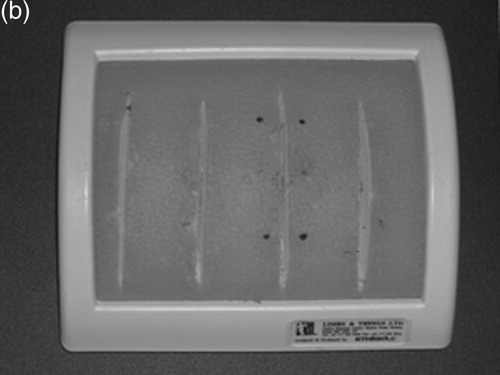
Figure 2. (a) Assembly used for Task 1, (b) suture pad used for Task 2, (c) target dots for Task 2, and (d) cutting grid used for Task 3.
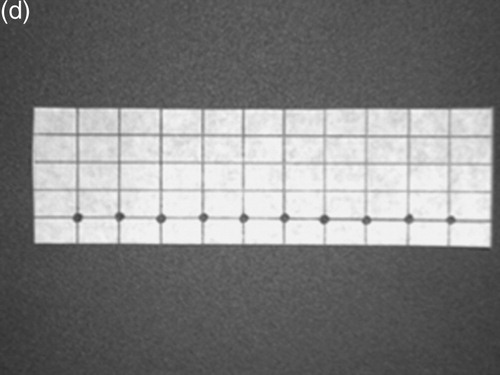
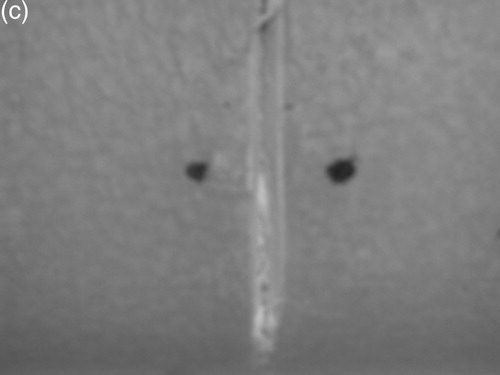
Task 2 was a suturing task where each surgeon had to place a single interrupted suture to approximate the cut edges of a silastic suturing pad. Two dots 1 mm in diameter were placed on a suturing pad ( and ) to mark where the suture had to be placed. The pad was secured inside a laparoscopic trainer. Using robotic needle drivers and 2-0 silk on a curved needle, each surgeon placed an interrupted suture with two throws on the pad. As in Task 1, the clock was started when the needle was properly positioned in the driver and was stopped when the last throw was secured. An error was scored for a dropped suture, a broken suture, or if the surgeon missed the targets and deviated out of the dot.
Task 3 involved cutting a piece of graph paper fastened to the suturing pad located inside the laparoscopic trainer. The graph paper contained 10 dots placed 10 mm apart and 10 mm from the bottom (). Starting at the first dot on the right and using a robotic grasper and curved scissors, the paper was grasped in the square on the left of the first dot. The cut was started on the right of the dot and completed inside the dot. This process was repeated for 10 dots. The process was monitored and an error was recorded each time a cut missed the targeted dot or if the graph paper was missed or torn when grasping or cutting.
Statistical analysis
The data were analyzed using Minitab v13 (Minitab Inc., State College, PA). A general linear model was used to evaluate and compare the task completion time (TCT) in seconds during different latencies, surgeons, tasks, and replications. A 5% level of significance was used to judge whether a factor or interaction between factors was statistically significant.
Results
Ability to complete the tasks
Interaction between different variables
All tasks were completed by all five surgeons at all four latencies. Analysis of TCT demonstrated that there was a significant interaction between surgeon and type of task (F = 2.15, p < 0.001), surgeon and different latencies (F = 6.91, p = 0.033), and type of task and different latencies (F = 2.37, p = 0.033). There were no interactions between repetition of tasks and any of the other three variables: surgeon, type of task, and latency. demonstrates the interaction plot for TCT scores.
Figure 3. Interaction plot for task time completion scores.
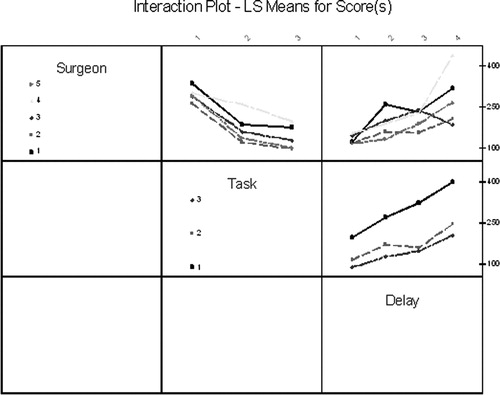
The impact of latency on TCT
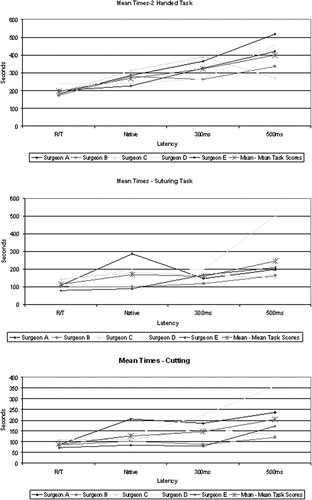
There was a significant increase in completion time for each task as the latencies increased from real-time to 500 ms (). The changes in completion time were not equal for each surgeon and for each task.
Figure 4. The effect of latency on TCTs.
Errors
Interaction between factors
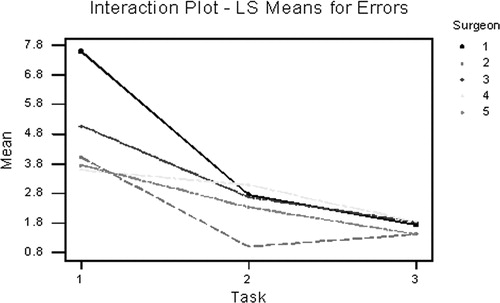
Analysis of errors observed during each task at different latencies demonstrated an interaction between surgeon and task (F = 4.40, p < 0.001) but no interaction between surgeon and latency or different task and latency or repetition as individual factors. shows the interaction plot for errors between surgeon and task.
Figure 5. Interaction plot for errors between surgeon and task.
Impact of delay on errors
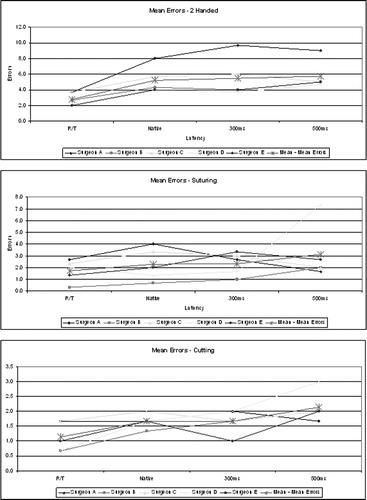
There was a significant increase in errors with increasing latencies (F = 9.81, p < 0.001), as shown in . There was also a significant difference in errors between surgeons at each latency over all three tasks (F = 7.30, p < 0.001), and a significant difference in errors between the three tasks (F = 63.31, p < 0.001).
Figure 6. The effect of latency on error rate.
Correlation between completion time and errors
There was a significant correlation between completion time for each task and error rate at each latency encountered with a Pearson correlation of 0.776 (p < 0.001).
Discussion
There has been a considerable amount of confusion surrounding the use of the term telerobotic surgery in the literature. The term has been used to describe scenarios varying from simple robotic surgery (Zeus or DaVinci), where the robot is connected to the surgeon's console via cables Citation[2–5], to telecollaboration Citation[2], Citation[6], where an expert surgeon can control a surgical robotic arm used to maneuver the camera view to assist and proctor another surgeon situated remotely Citation[7] (Socrates, Computer Motion Inc.), and telemanipulation, where one surgeon controls a surgical robotic arm and uses it to insert needles or other surgical instruments Citation[8], Citation[9]. However, it is important that these uses be distinguished from true telepresence remote surgery in which the remote surgeon performs two-handed surgical procedures using a multi-armed robotic surgical system. Consequently, the authors prefer the term ‘RARTS’ to describe this specialized application of telerobotic surgery. Currently, there is only one robotic system (Zeus TS, Computer Motion Inc.) capable of allowing the surgeon to control all three robotic arms via commercial telecommunication lines. Using this system, the only human RARTS cases have been performed by Professor Marescaux and his team on 7th September 2001 (Lindbergh operation) Citation[1] and by our team beginning on 28th February 2003 with two cases of telerobotic remote laparoscopic Nissen fundoplication between Hamilton, Ontario, and North Bay, Ontario Citation[10]. To date, 22 remote telepresence surgeries between the two Ontario sites have been performed, including 13 laparoscopic Nissen fundoplications, three laparoscopic right hemicolectomies, one laparoscopic anterior resection, three laparoscopic sigmoid resections, and two laparoscopic hernia repairs Citation[11].
The findings of our study suggest that latency is an important feature of RARTS, impacting on the ability of a surgeon to complete a task and on the accuracy with which the task is completed. This confirms the results of earlier experiments assessing the impact of latency on telemanipulation, which found that surgeons were able to perform tasks at latencies up to 700 ms, but with increased TCT and error rate Citation[12], Citation[13]. The study also demonstrates a significant difference between surgeons in the performance of various tasks during increasing latency. Whether this is solely dependent on level of experience or whether it is associated with the surgeons' innate ability was not tested in this study. It would be expected that both factors should play a role. If so, some surgeons may be more likely to successfully operate under conditions of high latency.
Our study demonstrated that there was no obvious cut-off at 300 ms with respect to the surgeons' ability to perform a task. However, we did not test the clinical implications of our finding. It would be important to understand whether the increased TCT and errors encountered during higher latencies would allow a surgeon to perform a remote telepresence surgery safely. We know from Professor Marescaux's experience that at 155 ms delay, he could safely perform a robotic-assisted laparoscopic cholecystectomy Citation[1]. We have also recently successfully performed a series of robotic-assisted remote laparoscopic Nissen fundoplications, colon resections, and hernia repairs at a latency of 135 ms. Our group intends to perform RARTS at higher latencies over the next year. Although latencies of over 500 ms were not tested, we also plan to repeat these studies at latencies of 750 ms and 1 s. Furthermore, we also intend to evaluate the impact of training, experience, and scaling of movement on the ability to perform robotic-assisted remote telepresence tasks at higher latencies.
In conclusion, this study demonstrates that although latency impacts on the ability of the surgeon to perform surgical tasks, it may still be possible to operate at higher latencies of up to 500 ms.
Acknowledgment
The authors acknowledge the assistance of Catherine Gill Pottruff and Paula McKay in the preparation of the manuscript.
References
- Marescaux J, Leroy J, Rubino F, Smith M, Vix M, Simone M, Mutter D. Transcontinental robot-assisted remote telesurgery: Feasibility and potential applications. Ann Surg 2002; 235(4)300–301
- Ballantyne G H. Robotic surgery, telerobotic surgery, telepresence and telementoring. Review of early clinical results. Surg Endosc 2002; 16(10)1389–1402
- Melvin W S, Needleman B J, Krause K R, Schneider C, Wolf R K, Michler R E, Ellison E C. Computer-enhanced robotic telesurgery. Initial experience in foregut surgery. Surg Endosc 2002; 16(12)1790–1792
- Ruurda J P, Broeders I A. Robot-assisted laparoscopic intestinal anastomosis. Surg Endosc 2003; 17(2)236–241
- Talamini M, Campbell K, Stanfield C. Robotic gastrointestinal surgery: Early experience and system description. J Laparoendosc Adv Surg Tech A 2002; 12(4)225–232
- Link R E, Schulam P G, Kavoussi L R. Telesurgery. Remote monitoring and assistance during laparoscopy. Urol Clin North Am 2001; 28(1)177–188
- Kavoussi L R, Moore R G, Partin A W, Bender J S, Zenilman M E, Savata R M. Telerobotic assisted laparoscopic surgery: initial laboratory and clinical experience. Urology 1994; 44(1)15–19
- Ruurda J P, van Vroonhoven T J, Broeders I A. Robot-assisted surgical systems: A new era in laparoscopic surgery. Ann R Coll Surg Engl 2002; 84(4)223–226
- Rovetta A, Sala R. Execution of robot-assisted biopsies within the clinical context. J Imag Guid Surg 1995; 1(5)280–287
- Pirisi A. Telerobotics brings surgical skills to remote communities. Lancet 2003; 361: 1794–1795
- Anvari M, McKinley C. Routine use of telerobotic remote surgery. Surg Endosc 2004; 18(Suppl.)(S180), (Abstract)
- Fabrizio M D, Lee B R, Chan D Y, Stoianovici D, Jarrett T W, Yang C, Kavoussi L R. Effect of time delay on surgical performance during telesurgical manipulation. J Endourol 2000; 14(2)133–138
- Thompson J M, Ottensmeyer M P, Sheridan T B. Human factors in telesurgery: Effects of time delay and asynchrony in video and control feedback with local manipulative assistance. Telemed J 1999; 5(2)129–137