Sirs,
Modalities for the treatment of striae distensae include topical tretinoin, intense pulsed light, the 585-nm pulsed dye laser, the 578-nm copper bromide laser, and non-ablative radio-frequency therapy (Citation1–7). Also, non-ablative 1550-nm erbium-doped fractional photothermolysis (FP) has proved its effectiveness and safety in patients with striae distensae (Citation8,Citation9); however, pronounced clinical improvement appears to require multiple treatment sessions. In Asian patients, postinflammatory dyschromia developing after ablative laser therapy has always been a concern; especially with lesions other than the face. Nouri et al. (Citation10) concluded that patients with skin types IV–VI should avoid carbon dioxide (CO2) laser treatments of striae, although the CO2 laser could theoretically stimulate the fibroblast activity and improve the lesions by controlled abrasion of the skin.
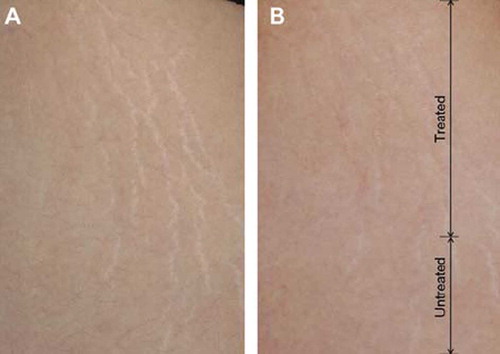
A 27-year-old Korean woman with Fitzpatrick type IV skin presented a striae alba on the anterior thigh, which occurred at the age of 13 years. On her initial presentation to our clinic, the patient showed several hypopigmented and atrophied lesions with irregular surfaces and textural changes (). She had neither a remarkable past medical history, including keloid and hypertrophic scars, nor a specific treatment history for the lesions of striae alba.
Figure 1. Clinical improvement of the striae alba after two sessions with the ablative 10 600-nm carbon dioxide fractional laser system: (A) before and (B) after the treatment. The laser therapy delivered was confined to the upper two-thirds of the lesion.
After obtaining informed consent, she was treated with two sessions of CO2 fractional laser (FS) using the Ultrapulse® Encore™ laser (Lumenis Inc., Santa Clara, CA, USA) with 4 weeks of elapsed time between treatments. For local anesthesia, the lesion was cleansed with 70% alcohol and topical EMLA cream (eutectic mixture of 2.5% lidocaine HCl and 2.5% prilocaine; AstraZeneca AB, Södertälje, Sweden) was applied under an occlusion an hour prior to laser treatment. At each treatment session, the laser fluences were delivered on two-thirds of the upper lesion with Deep FX™ mode at settings of 15 mJ, density 2, and 300 Hz.
The patient was prescribed prophylactic oral antibiotics for 3 days. She was instructed to use Cicaplast® (La Roche-Posay, Paris, France) for a month after each treatment session to promote wound healing and prevent dryness, and was also recommended to avoid overexposure to sunlight. A photograph was taken 2 months after the last treatment () and the lesions of striae alba were noticeably improved after the two treatments compared with the untreated area. The patient showed satisfaction with the results and complained of no adverse effects.
The CO2 laser has been widely used for treating various epidermal and dermal lesions. Nowak et al. (Citation11) described that the CO2 laser enhances fibroblast replication, stimulates basic fibroblast growth factor secretion, and reduces transforming growth factor β1 secretion. However, because of the possibility of pigmentary alteration, the use of ablative laser is limited to patients with dark skin (Citation10).
Fractional laser technology decidedly shortens the recovery time and reduces the risk of adverse events by leaving an intact epidermal architecture surrounding each coagulated microthermal treatment zone. By adopting CO2 on the advanced technology of the fractional laser system, CO2 FS can be expected to obtain the effect of ablative laser more safely. A previous report demonstrated that post-therapy hyperpigmentation had developed in two of 15 participants after three sessions of CO2 FS treatment on facial lesions; neither immediate nor delayed post-therapy hypopigmentation was discovered (Citation12).
In present study, the Deep FX mode was used to deliver laser energies to deeper portions of the scar tissue than Active FX™ mode. Moreover, by the fact that the total treatment zone is broader with Active FX than with Deep FX, with a spot size of 1.25 mm versus 0.12 mm, respectively, downtime is shorter with Deep FX. The therapeutic effect of CO2 FS on striae alba was easily comparable because the laser was delivered and confined to the upper two-thirds of the lesion in our patient. We would like to emphasize that our patient, an Asian patient with Fitzpatrick skin type IV, did not present noticeable adverse events, especially aggravation of the striae alba and post-therapy hyper- or hypopigmentation – even with the lesion located on an area other than the face.
Acknowledgement
The authors have declared no conflicts of interest and no funding sources.
References
- Kang S, Kim KJ, Griffith CE, Wong TY, Talwar HS, Fisher GJ, . Topical tretinoin (retinoic acid) improves early stretch marks. Arch Dermatol. 1996;132:519–26.
- McDaniel DH, Ash K, Zukowski M. Treatment of stretch marks with the 585-nm flashlamp-pumped pulsed dye laser. Dermatol Surg. 1996;22:332–7.
- McDaniel DH. Laser therapy of stretch marks. Dermatol Clin. 2002;20:67–76.
- Hernandez-Perez E, Colombo-Charrier E, Valencia-Ibiett E. Intense pulsed light in the treatment of striae distensae. Dermatol Surg. 2002;28:1124–30.
- Jimenez GP, Flores F, Berman B, Gunja-Smith Z. Treatment of striae rubra and striae alba with the 585-nm pulsed dye laser. Dermatol Surg. 2003;29:362–5.
- Longo L, Postiglione MG, Marangoni O, Melato M. Two-year follow-up results of copper bromide laser treatment of striae. J Clin Laser Med Surg. 2003;21:157–60.
- Suh DH, Chang KY, Son HC, Ryu JH, Lee SJ, Song KY. Radiofrequency and 585-nm pulsed dye laser treatment of striae distensae: A report of 37 Asian patients. Dermatol Surg. 2007;33:29–34.
- Stotland M, Chapas AM, Brightman L, Sukal S, Hale E, Karen J, . The safety and efficacy of fractional photothermolysis for the correction of striae distensae. J Drugs Dermatol. 2008;7:857–61.
- Kim BJ, Lee DH, Kim MN, Song KY, Cho WI, Lee CK, . Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9:33–7.
- Nouri K, Romagosa R, Chartier T, Bowes L, Spencer JM. Comparison of the 585-nm pulsed dye laser and the short pulsed CO2 laser in the treatment of striae distensae in skin types IV and VI. Dermatol Surg. 1999;25:368–70.
- Nowak KC, McCormack M, Koch RJ. The effect of superpulsed carbon dioxide laser energy on keloid and normal dermal fibroblast secretion of growth factors: A serum-free study. Plast Reconstr Surg. 2000;105:2039–48.
- Chapas AM, Brightman L, Sukal S, Hale E, Daniel D, Bernstein LJ, . Successful treatment of acneiform scarring with CO2 ablative fractional resurfacing. Lasers Surg Med. 2008;40:381–6.