Sirs,
Introduction
The ThermaCool® system (Thermage®, Inc., Hayward, CA, USA) is a non-invasive, non-ablative device that uses monopolar radio-frequency (MRF) energy to tighten the skin (Citation1). Since its approval by the US Food and Drug Administration in 2002 for rhytides, there have been a number of publications on monopolar RF with data supporting its clinical efficacy (Citation2). However, little is known of Thermage in Asian skin.
It is generally recognized that Asian and European skin age differently. With a greater elastic nature and solar protection, there is a delayed onset of wrinkles in Asians (Citation3). Instead, the Asian face tends to age principally due to gravitational descent. The thicker dermis with a greater amount of collagen, heavier malar fat pad, and weaker skeletal support all contribute to considerable facial sagging compared to Caucasians (Citation4). Owing to the differences in the intrinsic properties of the skin, MRF may not be equally effective in Asians and Caucasians. In this study, the general opinion of dermatologists practicing Thermage in Asians is described to better understand its indications, benefits and limitations in Asian skin.
Methods
A Thermage questionnaire, consisting of 13 questions, was distributed to dermatologists who had had more than 2 years of experience or had treated more than 100 patients using Thermage. Dermatologists who attended the annual Thermage user meeting were asked about their experience with the device, and those who met the criteria above were invited to answer the questionnaire. A total of 60 questionnaires were handed out and we evaluated the 48 that were returned (). Among those who answered the questionnaire, 83% replied that they use ThermaCool TC™ (the first generation Thermage) and 17% use ThermaCool NXT™. A total of 8% had experience with both devices.
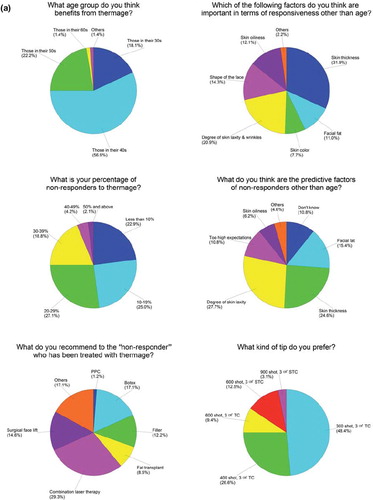
Figure 1. (A and B) The response to the questionnaire based on the 48 surveys returned.

Results and Discussion
According to our group of dermatologists, Asians in their 40s (56.9%) were considered to benefit most from Thermage followed by those in their 50s (22.2%) and 30s (18.1%). In previous literature, Thermage has been suggested to be ideal for patients in their 30s with possible extension to the mid-40s (Citation5). Such a difference may be attributed to the fact that skin aging features progress differently between Asians and Caucasians. In a particular study, the wrinkle onset was found to be delayed by 10 years in Chinese women as compared to French women (Citation3).
Skin thickness (31.9%) and the degree of skin laxity and wrinkles (20.9%) were chosen as the two most important factors in terms of responsiveness to Thermage, followed by face shape (14.3%), skin oiliness (12.1%), facial fat (11.0%) and skin color (7.7%). Many preferred thin (48.1%) to average (29.6%) skin thickness, average facial fat (80%), an oval-shaped face (69.2%), average (27.3%) to oily skin (63.6%) and a light (85.7%) skin tone. As MRF targets the dermis for skin tightening, it is natural that skin tightening would be more obvious in a person with skin of thin to average thickness and there is no doubt that mild-to-moderate skin laxity responds better to Thermage. The Asian face ages principally due to gravitational descent, where the thicker skin, heavier malar fat pad, and weaker skeletal support all contribute to considerable facial sagging. An oval-shaped face and a moderate amount of facial fat may lower the risk of early facial sagging and give a synergistic effect to Thermage.
A total of 28.9% of dermatologists replied that 20–29% of patients were non-responders. Patients usually made a follow-up visit 3 and 6 months after Thermage for both subjective (patient's satisfaction) and objective (clinical examination and photographic analysis by the doctor) assessment. As predictive factors of non-responders other than age, definite skin laxity, thick skin and too high expectations were quoted, with 10.8% having no clue whatsoever. A surgical face lift (14.6%) and combined laser therapy (29.3%) were recommended to non-responders followed by Botox (17.1%), fillers (12.2%) and fat transplant (8.5%).
The interval between Thermage treatments was mainly 1 year and above (62.7%), with the majority using a 300-shot 3 cm2 TC tip (48.4%) or a 400-shot 3 cm2 TC tip (26.6%). The difference in the degree of skin laxity may account for the lower number of shots performed in Asians compared to Caucasians where 600–800 firings are usually made (Citation5). The treatment levels performed in Asians were comparable to Caucasians, with the majority being treated at level 4–4.5 (32.4%) and 3–3.5 (32.4%).
Other than wrinkles and skin laxity, improvement in acne (50%) and rosacea (16.7%) was observed. Some also experienced a transient but definite decrease in sebum output. Improvement in skin tone and acne reduction does not seem to be limited to Asian skin as it has been suggested in previous studies (Citation1).
The complication rate of Thermage was low, with most being minor and easily managed with simple dressing or observation. However, fat atrophy has been reported, which required filler injections subsequently. Compared to the initial ThermaCool TC device, complications are now rare with ThermaCool NXT.
Overall, Asians in their 40s and 50s and those with thin skin, a moderate amount of fat and an oval-shaped face seem to benefit most from Thermage under the common protocol of 300–400 firings at levels 3–4.5 and an interval of more than 1 year. Although such patients are theoretically the best Asian candidates, this should only be taken as a reference as it does not always guarantee response. Further well-designed studies are needed to assess not only effectiveness but also to clarify the best treatment protocol.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Abraham MT, Mashkevich G. Monopolar radiofrequency skin tightening. Facial Plast Surg Clin North Am. 2007; 15:169–177.
- Burns AJ, Holden SG. Monopolar radiofrequency tissue tightening—how we do it in our practice. Lasers Surg Med. 2006;38:575–579.
- Nouveau-Richard S, Yang Z, Mac-Mary S, Li L, Bastien P, Tardy L, . Skin ageing: A comparison between Chinese and European populations. A pilot study. J Dermatol Sci. 2005;40:187–193.
- Shirakabe Y, Suzuki Y, Lam SM. A new paradigm for the aging Asian face. Aesthetic Plast Surg. 2003;27:397–402.
- Hodgkinson DJ. Clinical applications or radiofrequency: Nonsurgical skin tightening (thermage). Clin Plast Surg. 2009;36:261–268.