
To the Editor:
We are grateful for Professor Bateman's interest and insightful comments. We fully agree that the ongoing assessment of a patient with hepatotoxicity following paracetamol overdose should include monitoring international normalized ratio or INR, and creatinine and bilirubin levels in addition to transaminase concentrations. We excluded patients meeting the Kings College Hospital criteria,Citation1 and we suggest that the ratio of aspartate aminotransferase (AST) to alanine aminotransferase (ALT) may be useful only in patients with elevated transaminase concentrations in the absence of other laboratory or clinical evidence of hepatic failure.
We acknowledge that AST is not as tissue-specific as ALT.Citation2,Citation3 One of us (MEM) is old enough to recall using serial AST (then known as “serum glutamic oxaloacetic transaminase or SGOT”) as part of the laboratory evaluation of possible myocardial infarction before troponin became the preferred marker of myocardial injury. We excluded patients with alternative causes of transaminase elevation, such as rhabdomyolysis. Our data only apply to patients with confirmed paracetamol overdoses in which the liver is the clear source of transaminase elevation.
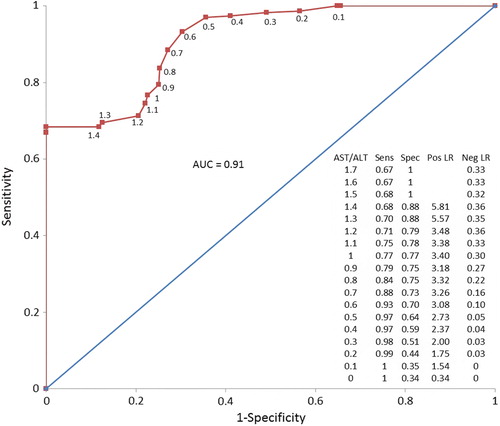
None of the patients in our cohort had a decline in ALT followed by clinical deterioration. Further, our analysis of the AST/ALT ratio to identify falling ALT concentrations () is similar to our original analysis of the ability of the ratio to identify falling AST concentrations.
Fig. 1. Receiver operating characteristic (ROC) curve for AST/ALT ratio in identifying a pair of AST and ALT concentrations as occurring after the observed peak ALT. Data labels indicate the AST/ALT ratio for each point in increments of 0.1. The trapezoidal area under the curve is 0.91. The embedded table shows the sensitivity (Sens), specificity (Spec), positive likelihood ratio (Pos LR), and negative likelihood ratio (Neg LR) for each cut-off point of AST/ALT ratio (colour version of this figure can be found in the online version at www.informahealthcare.com/ctx).
Our findings are not generalizable to practice settings which routinely measure only one transaminase (neither AST or ALT). Without having both transaminase concentrations, one cannot calculate the ratio. In the US, AST and ALT levels are both elements of the comprehensive metabolic panel (CPT code 80053) and hepatic function panel (CPT code 80076),Citation4 so both enzyme concentrations are consistently available together in patients in the US. However, the Canadian Acetaminophen Overdose Study (CAOS) database illustrates that this has not been consistently true elsewhere. Many patients in the CAOS database had measured either AST or ALT, but not always both. In research using transaminase concentrations in devising better methods of prognosis for paracetamol overdose patients, CAOS investigators have used AST and ALT nearly interchangeably as aminotransferases (ATs).Citation5,Citation6 While our data illustrate that AST and ALT have similar values as concentrations are rising, our data also show that AST and ALT are not equivalent as their respective concentrations fall.
While microRNA-122 shows considerable promise in the assessment of hepatic injury after paracetamol overdose,Citation7 this test is not yet widely available for clinical use.
Declaration of interest
The authors report no declarations of interest. The authors alone are responsible for the content and writing of the paper.
References
- O’Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 1989; 97:439–445.
- Ramaiah SK. A toxicologist guide to the diagnostic interpretation of hepatic biochemical parameters. Food Chem Toxicol 2007; 45:1551–1557.
- Ozer J, Ratner M, Shaw M, Bailey W, Schomaker S. The current state of serum biomarkers of hepatotoxicity. Toxicology 2008; 245:194–205.
- US Department of Health and Human Services. Centers for Medicare and Medicaid Services. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R1451CP.pdf. Accessed on 21 February 2015.
- Sivilotti MLA, Yarema, MC, Juurlink DN, Good AM, Johnson DW. A risk quantification instrument for acute acetaminophen overdose patients treated with N-acetylcysteine. Ann Emerg Med 2005; 46:263–271.
- Green TJ, Sivilotti ML, Langmann C, Yarema M, Juurlink D, Burns MJ, Johnson DW. When do the aminotransferases rise after acute acetaminophen overdose? Clin Toxicol 2010; 48:787–792.
- Antoine DJ, Dear JW, Lewis PS, Platt V, Coyle J, Masson M, et al. Mechanistic biomarkers provide early and sensitive detection of acetaminophen-induced acute liver injury at first presentation to hospital. Hepatology 2013; 58:777–787.