
Abstract
Background and purpose — Instability of the patellofemoral joint is a common disorder in children and young adults. Although it has multifactorial causes, a shallow femoral trochlea is the single most important factor for instability. There is no consensus as to the etiology of trochlear dysplasia. We assessed whether the presentation of the fetus at birth could be a predisposing factor for trochlear dysplasia.
Subjects and methods — We examined 348 knees in 174 newborns using ultrasonography, concentrating especially on the trochlea femoris. We measured the sulcus angle (SA) on a transverse scan. The way of fetal presentation at birth and standard parameters such as sex, gestational age, and length and weight at birth were registered. As breech presentation is a known risk factor for dysplasia of the hip, we also looked for an association between dysplasia of the femoral trochlea and dysplasia of the hips.
Results — The mean SA was 148°. 17 knees in 14 children had an SA of >159°, which was defined as the threshold value for dysplasia. The incidence of breech position in these children was 15-fold higher. Of the different groups of breech positions, a child in frank breech with the knees locked in extension had a 45-fold increased risk of having trochlear dysplasia.
Interpretation — For some newborns, a high sulcus angle can be found at birth, indicating that trochlear dysplasia can be found from birth. Breech presentation with knees extended appears to be a major risk factor for development of trochlear dysplasia.
Dysplasia of the femoral trochlea is a major predisposing factor for instability of the patellofemoral joint (Dejour et al. Citation1994, Hawkins et al. Citation1986). There is no consensus as to whether it is genetic in origin (Glard et al. Citation2005), caused by imbalanced forces indicating maltracking and remodeling of the trochlea during infancy and growth (Nietosvaara Citation1994), or due to other unknown factors. Breech presentation is a known risk factor for hip dysplasia (Holen et a. 1996). Knowing this made us wonder whether birth presentation could also be a predisposing factor for trochlear dysplasia. The general shape of the adult bones of the knee is determined early in pregnancy (Walmsley Citation1940) and the morphology of the fetal femoral sulcus is comparable with its shape in adults (Glard et al. Citation2005). A high sulcus angle (SA) and a low trochlear depth (TD) are parameters that are used to describe dysplasia of the adult femoral trochlea. Ultrasonography has proven useful for examination of the femoral trochlea in newborns, allowing measurement of both SA and TD. The SA was found to be the most reliable parameter, with an intra-examiner variation of −1° (SD 2.5) and an inter-examiner variation of 0° (SD 2.1) (Øye et al. 2015). We examined the knees of 174 newborns using ultrasonography, concentrating especially on the femoral trochlea. There are great variations in SA in newborns, and we have suggested a cut-off angle for dysplasia of 159° (Øye et al. 2015). Based on our previous experience of using ultrasound to obtain anthropometric measurements in newborns, we chose this modality to evaluate possible risk factors for trochlear dysplasia. Our aim was to determine whether birth presentation, as an indicator of the intrauterine positioning of the fetus at the last stage of pregnancy, could be a possible risk factor for femoral dysplasia in the newborn.
Subjects and methods
Subject selection and demographic data
To our knowledge, no other studies of the trochlea femoris in newborns have provided us with the information needed for sample size calculations. As an explorative cohort study, the size of our study population was based on practical considerations. Ultrasound examinations of both knees of all newborns admitted to 1 of 3 obstetric wards in the same hospital were performed over 2 months in 2010. Of 178 newborns assessed for eligibility, the parents of 4 declined participation. All the other parents gave their informed consent to participate in the study. The examinations were performed at Trondheim University Hospital, Norway, which manages around 3,800 births annually. All the newborns were examined by the same person within 3 days of birth regardless of other conditions, except those requiring treatment in the intensive care unit. We registered the following data: sex, length, weight, gestational age, hip status, and birth presentation.
Ultrasonography
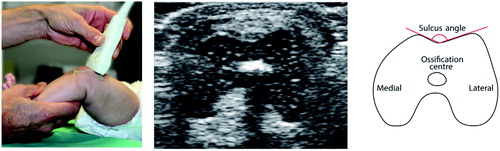
Ultrasound examinations were performed with the child in his or her bed or in a comfortable position beside the mother. The child was positioned supine and a portable ultrasound scanner (GE Logiq Book XP; GE Medical Systems Co., Jiangsu, China) with a linear GE 8L probe was used. Many of the children slept through the examination, and none expressed pain or substantial discomfort. To position the patella distal to the ventral point of the lateral facet, the knee was flexed over 45°. The transducer was first held in a transverse plane perpendicular to the axis of the femoral diaphysis. By moving the transducer caudally distal to the epiphysis, the trochlea and its most ventral point were defined. Images were produced by holding the transducer perpendicular to the femoral axis. The femoral ossification center had to be visualized, serving as a guide for correct perpendicular angulation of the probe (). With the knee still in flexion and the transducer held in the sagittal plane, an image with the patella and the patellar ligament was obtained.
Figure 1. Collage demonstrating ultrasound examination of the knee of a 3-month-old girl, with a corresponding ultrasound screenshot and a line diagram for illustration of the sulcus angle (SA). With the knee flexed above 45° and the transducer held in a transverse plane perpendicular to the axis of the femoral diaphysis, an image of the femoral condyles with the trochlea was produced. The femoral ossification center is visible.
Ultrasonographic parameters
Various parameters have been used to describe the anatomy of the femoral trochlea. The sulcus angle (SA) is the closed angle defined by the intersection of the lines parallel to the articular cartilage of the medial and lateral femoral facets. It is easy to measure and interpret and is commonly used to describe dysplasia of the femoral trochlea. In addition to the SA, we recorded other parameters. One of them, trochlear depth (TD), is generally accepted as a measure of dysplasia. Others, such as the trochlear area (TA) and the trochlear index (TI), were parameters designed for our population to see if we could find one paremeter more accurate and suitable for use when examining newborns. Of these parameters, the SA proved to be the most reliable one for distinguishing a dysplastic trochlea from a normal one (Øye et al. 2015) (). The patellar height described by the Insall-Salvati index was calculated by dividing the length of the patellar tendon by the length of the patella.
Demographic parameters
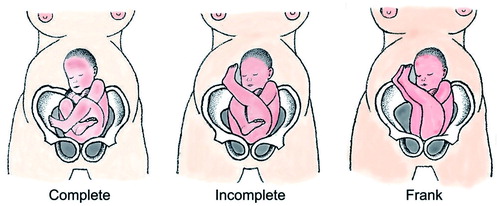
From 28–30 weeks’ gestation, the position of the fetus is in one of these categories: cephalic, breech, or transverse. We categorized the presentation of the fetus at birth as cephalic, breech, or transverse/unknown. Breech position was further categorized into complete, incomplete, or frank ().
Figure 2. The different categories of breech position. Complete breech is where the knees are held in a fixed flexed position. Incomplete breech is where one knee is kept flexed while the other is extended. The most frequent type is the frank breech position, where the knees are fixed extended while the hips are flexed.
As a consequence of our screening for hip dysplasia, newborns are tested for instability of the hip using the Ortolani test. Those testing positive, or others with known risk factors for hip dysplasia, are examined with ultrasonography of the hip joint after birth. Our study population was categorized into the following subgroups with regard to their hip joint status: normal, dysplastic, subluxed, luxated, unstable, doubtful, or irregular caput femoris.
Statistics
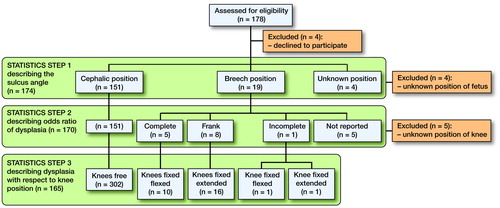
All statistical calculations were performed using IBM SPSS Statistics version 21. Visual inspection of Q-Q plots was used to determine whether data were normally distributed. The sulcus angle measurements were normally distributed. The statistical analyses were performed in 3 steps (). First, all 174 children were included when presenting the descriptive statistics. A paired-samples Student t-test was used when comparing sulcus angle measurements from left and right knees and an independent Student t-test was used when comparing sulcus angle measurements between sexes. Secondly, as birth presentation was believed to be a significant variable, children with unknown presentation were removed from the analysis and the remainder (n = 170) were included in the regression analysis that followed. Finally, knees of unknown position were removed and the remainder (n = 330) were included when describing the odds ratio for dysplasia with respect to knee position.
Figure 3. Flow chart illustrating the statistical analyses. These were performed in 3 main steps. In the first step, all 174 children were included, The sulcus angle (SA) was analyzed as a continuous variable. In the second step, 4 children with unknown birth presentation were excluded from further analysis. The SA was analyzed as a dichotomous variable when describing the odds ratio for dysplasia with respect to birth presentation. In the final step, knees of unknown position were excluded to obtain the odds ratio for dysplasia with respect to knee position.
Mixed linear models were used to account for data dependency caused by examination of bilateral knees. Initially, the parameters sex, length, weight, and gestational age were considered as possible covariates. Directed acyclic graphs were then used to identify the ones needed to be included in the models (Shrier and Platt Citation2008). Length and weight were finally selected. The residuals in the models were found to be normally distributed. The dependent variable (SA) was dichotomized (dysplastic or non-dysplastic). Generalized mixed linear models with the same nested study design were used when analyzing dichotomous data. First, the birth presentation was used as explanatory variable with weight as a covariate included in the analysis. Then, knee position was used as explanatory variable with no covariates included. The level of significance was set at p ≤ 0.05.
Ethics
The study was approved by the Regional Committees for Medical and Health Research Ethics (REC) and by the review board at our department (2010/160-2).
Results
The mean gestational age of the study population was 39 weeks (SD 3.5), the mean birth weight was 3,476 g (SD 562), and the mean birth length was 49 cm (SD 2.7). The grand mean sulcus angle was 148° and 17 children had a sulcus angle of >159°. The mean difference between the left and right knees was not statistically significant (0.3°; p = 0.7). Consequently, data from both sides were pooled in the descriptive results. There was a significant difference been the sexes (p = 0.05) and the results are presented separately (). The presentation at birth had a statistically significant influence on sulcus angle. Weight was statistically significant and length was not ().
Table 1. Measurement data including the grand mean sulcus angle (SA) and the sulcus angle according to gender
Table 2. Statistics step 1. Presentation of the parameters and their statistical significance. Overall, children born in breech position had a sulcus angle that was 3.8 degrees higher than those born in cephalic position
The knees were divided into 2 groups, dysplastic or not. Children born with breech presentation carried a 15-fold higher risk of having trochlear dysplasia than children born with cephalic presentation. The child’s weight had no statistically significant effect ().
Table 3. Statistics step 2. Odds ratio of dysplasia. Patients with unknown birth position were excluded (n = 4). The sulcus angle was analyzed as a dichotomous variable. Breech presentations had a 15-fold higher risk of dysplasia
Cross-tabulations between the position of the fetus and knee position according to dysplasia are presented in . A child born with the knees in a fixed extended position had a 45-fold higher risk of having trochlear dysplasia (95% CI: 13–165) than those born with the knees in a free or flexed position. 1 child presented with an incomplete breech position, with the right knee in extension and the left in flexion. The SA for the right knee was 159° and it was 146° for the left knee.
Table 4. Cross-tabulation presenting dysplasia or no dysplasia, according to the position of the fetus and the knees
In this study, 2 hips were dysplastic and 2 were luxated. None of these children had knee dysplasia.
The axial position of the patella relative to the trochlea as shown by the Insall-Salvati index showed no correlation with the sulcus angle.
Discussion
In this study, 178 newborns were examined to determine whether birth presentation could be a possible risk factor for femoral trochlear dysplasia in the newborn. According to the Medical Birth Registry of Norway, our population had birth parameters that were very similar to the national mean values for birth weight and length (3,475 g and 50 cm, respectively), and are therefore representative of the neonatal population of Norway. Boys had a smaller sulcus angle than girls, and the difference of 1.7° is in accordance with results presented earlier (Oye et al. Citation2015). The presentation at birth had the greatest influence on sulcus angle. With a sulcus angle closer to 180° representing dysplasia, children with breech presentation had an angle that was approximately 4° higher, and consequently closer to a dysplastic condition. Length and weight were initially included as covariates. They had only a marginal influence on the sulcus angle and appear not to be of clinical importance.
A borderline of SA > 159° has been suggested for dysplasia (Oye et al. Citation2015). To further investigate the effect of presentation on dysplasia, we first excluded 4 children with unknown presentation before dichotomizing them into dysplastic and non-dysplastic groups. Statistically, presentation had a highly significant effect and children born in the breech position had an approximately 15-fold higher risk of dysplasia. However, we must emphasize that there was a wide 95% confidence interval, showing the uncertainty of this risk estimate.
The child’s birth presentation might also be a confounder regarding knee position. The most important factor could be whether or not the knee was extended. In the final analyses, 18 knees of unknown position were excluded. Gestational age was found to be statistically significant but hardly clinically significant. Knee position appeared to be most important. Knees in the extended position had a 45-fold higher risk of dysplasia than knees that were free to flex. Once more, the wide 95% confidence interval must be taken into account.
Based on our findings, the most important factor associated with trochlear dysplasia appears to be knee position at birth. Efforts are being made to discover the etiology of trochlear dysplasia, and our findings should provide new knowledge to answer this question. We are not aware of any other publications that have described the relationship between birth presentation, knee position, and trochlear dysplasia.
Awareness of the association between breech position and dysplasia of the hip has led to the practice of ultrasound screening after a breech delivery. In general, the majority of children born in the breech position have the legs extended, which has been shown to be the most unfortunate position regarding development of dysplasia of the hips (Holen et al. Citation1996). Only 4 children in the present study presented with hip dysplasia. The study sample was too small for formal statistical tests to be meaningful.
Breech presentations constitute 3–5% of all deliveries (Scheer and Nubar Citation1976). In 2010, 5.1% of deliveries at Trondheim University Hospital (196 of 3,818 newborns) were breech presentations; in 2011 this figure was 5.3%. This slightly raised incidence may be explained by the fact that as this is the main hospital in our region, with the expertise needed to handle premature deliveries and suspected difficult births, breech deliveries are admitted more frequently.
The modeling of the femoral trochlea can be compared with that seen in the hip (Bialik et al. Citation1999). Considering our findings, the shape of the fetal femoral trochlea appears to be susceptible to the influence of mechanical forces. A moving knee with normal patellar tracking in the final stage of pregnancy may be of vital importance in ensuring a normal anatomy. A fetus with space to kick and flex the lower limbs has a good prospect of developing a femoral trochlea with the depth needed to support the patella. In a future prospective clinical study, we may be able to use our knowledge of the ability of the immature trochlea to remodel to our advantage by controlling the forces acting upon the cartilage from the patella.
CRØ performed the examinations. OAF carried out the statistical analyses. CRØ drafted the manuscript. All the authors (CRØ, OAF, and KJH) contributed to interpretation of the analyses and revision of the manuscript.
The study was funded by grants from the Norwegian Orthopaedic Association and the Research Foundation of UNIMED (#97191).
- Bialik V, Bialik G M, Blazer S, Sujov P, Wiener F, Berant M. Developmental dysplasia of the hip: a new approach to incidence. Pediatrics 1999; 103(1): 93-9.
- Dejour H, Walch G, Nove-Josserand L, Guier C. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 1994; 2(1): 19-26.
- Glard Y, Jouve J L, Garron E, Adalian P, Tardieu C, Bollini G. Anatomic study of femoral patellar groove in fetus. J Pediatr Orthop 2005; 25(3): 305-8.
- Hawkins R J, Bell R H, Anisette G. Acute patellar dislocations. The natural history. Am J Sports Med 1986; 14(2): 117-20.
- Holen K J, Tegnander A, Terjesen T, Johansen O J, Eik-Nes S H. Ultrasonographic evaluation of breech presentation as a risk factor for hip dysplasia. Acta Paediatr 1996; 85(2): 225-9.
- Nietosvaara Y. The femoral sulcus in children. An ultrasonographic study. J Bone Joint Surg Br 1994; 76(5): 807-9.
- Oye C R, Holen K J, Foss O A. Mapping of the femoral trochlea in a newborn population: an ultrasonographic study. Acta Radiol 2015; 56(2): 234-43.
- Scheer K, Nubar J. Variation of fetal presentation with gestational age. Am J Obstet Gynecol 1976; 125(2): 269-70.
- Shrier I, Platt R W. Reducing bias through directed acyclic graphs. BMC Med Res Methodol 2008; 8: 70. doi: 10.1186/1471-2288-8-70.
- Walmsley R. The development of the patella. J Anat 1940; 74(Pt 3): 360-83.