Abstract
Objectives:
Advances in survival in multiple myeloma have focused payer attention on the cost of care. An assessment was conducted to compare the costs of two recent treatments for relapsed/refractory multiple myeloma (rrMM), from the perspective of a US payer.
Methods:
An economic model estimated the total costs of care for two guideline-recommended therapies in rrMM patients: bortezomib (BORT) and lenalidomide plus dexamethasone (LEN/DEX). To evaluate total treatment costs, the costs associated with drug treatment, medical resource utilization, and adverse event (AE) management were determined for each regimen over a common 1-year period. Medical costs and grade 3/4 AE costs were based on rates from published literature, package inserts, and fee schedules (US dollars). To evaluate cost per outcome, assessments determined the monthly costs without disease progression based on pivotal clinical trials (APEX [BORT] and MM-009/MM-010 [LEN/DEX]). Univariate sensitivity analyses and alternative scenarios were also conducted.
Results:
Drug costs for the treatments were very similar, differing by under $10 per day. Medical and AE management costs for BORT were higher by more than $40 per day. Treatment with BORT had annual excess total costs of >$17,000 compared with LEN/DEX. A cost advantage for LEN/DEX was maintained across a variety of sensitivity analyses. Total cost per month without progression was 11% lower with LEN/DEX.
Limitations:
This analysis relied on separate studies having similar comparators, populations, and end-points. Actual treatment patterns and costs pre- and post-relapse may vary from the base scenario and sensitivities modeled. The 12-month time frame captures the preponderance of costs for a relapse line of therapy, yet may not reflect the entirety of costs. There is insufficient evidence to determine whether, or how, a difference in the lifetime costs of the two regimens would vary from the 1-year cost difference.
Conclusion:
While rrMM treatment with BORT and LEN/DEX had comparable drug costs, total treatment costs for BORT were higher due to ongoing direct medical and AE management costs. Total costs per outcome (a month without disease progression) were lower for LEN/DEX.
Introduction
The treatment and outcome of patients with multiple myeloma (MM) has been transformed over the past decade by the introduction of therapeutic agents such as the immunomodulatory tumor-inhibiting agents thalidomide and lenalidomide (LEN), and the proteasome inhibitor bortezomib (BORT)Citation1. According to National Comprehensive Cancer Network (NCCN) guidelines, BORT and LEN are recommended as primary therapy in newly diagnosed MM (in combination with dexamethasone [DEX]; category 1) and as maintenance therapy (category 2A)Citation2. However, most MM patients eventually progress to relapsed or refractory MM (rrMM), and typically require one or more additional cycles of treatment or new regimensCitation3.
A variety of outcome measures have been used to assess treatment success, including response rates, time to progression (TTP), and overall survival (OS). A working group of the American Society of Hematology (ASH) and the US Food and Drug Administration (FDA) cited concerns using complete response (CR) as a primary clinical trial end-point, because biomarker test reliability is not well established and there is an unclear relationship with patient survivalCitation1,Citation4,Citation5. The working group recommended TTP and OS as more appropriate end-points. However, the use of OS as an end-point is complicated by the long duration of follow-up and large sample size required, and the potential of subsequent treatments (as cross-over or salvage) to confound the impact of the primary treatmentCitation6. In clinical trials, TTP may be a good predictor of survivalCitation5.
Both LEN and BORT have demonstrated rrMM efficacy in pivotal clinical trials based on TTP (primary end-point) and OS (secondary end-point)Citation1,Citation7–13. In a pooled analysis of studies MM-009 and MM-010, LEN/DEX patients achieved a substantially longer median TTP at 48 months follow-up (13.4 months) vs DEX-only patients (4.6 months; p < 0.001 for both trials)Citation8. Likewise, OS was significantly improved in the LEN/DEX group vs the placebo group in both studies (MM-009: hazard ratio [HR] for death, 0.66; p = 0.03; MM-010: HR, 0.44; p < 0.001)Citation13,Citation14. In the APEX trial, patients receiving BORT had a significantly longer median TTP vs DEX (6.2 vs 3.5 months; p < 0.001). Treatment with BORT was associated with an improved OS vs DEX (odds ratio: 0.57; p = 0.001)Citation11.
As survival in rrMM extends and treatment is prolonged, the costs of therapy have become increasingly important to payers and patients. This has led payers to seek an understanding of the full range of costs associated with treatment optionsCitation15. Research has been published attempting to evaluate the costs of rrMM treatmentCitation16–20. However, analyses should consider the total drug and medical costs associated with a specific therapy, as well as administration costs and adverse event (AE) management, over a consistent time horizon, in order to make a balanced assessment of the overall costs of careCitation16,Citation21,Citation22. As such, a comparison of the total annual costs associated with LEN/DEX and BORT in patients with rrMM was undertaken from a US managed care perspective.
Methods
Model design
An economic model evaluated the total treatment costs of LEN/DEX vs BORT for rrMM patients in a US managed care plan. Direct medical costs were modeled over a common 1-year period, starting with the initiation of treatment for rrMM and ending 12 months later.
Treatment regimen data, AE information, and information on expected TTP in rrMM for LEN and BORT were obtained from three pivotal clinical registration trials (LEN/DEX: MM-009, MM-010; BORT: APEX)Citation11,Citation13,Citation14. Dosage and administration inputs were obtained from FDA-approved prescribing information for LEN and BORTCitation23,Citation24. Medical and AE management costs were based on a prior economic analysis of LEN and BORT and other published literatureCitation10. In addition, to evaluate costs in the context of clinical outcomes, an analysis was performed to calculate treatment costs/month without disease progression.
Model inputs: treatment regimen and costs
Both treatment regimens were assessed over a 12-month period in the base-case scenario. Treatment resource utilization was based on the dosing schedule from the respective clinical trials and labelsCitation14. Regimens for each treatment had treatment-day periods and non-treatment-day (rest) periods. For the model, the treatment-day LEN dose of one 25 mg capsule was taken from the labelCitation23. In APEX, BORT was administered as 1.3 mg/m2 IV on days 1, 4, 8, and 11 for eight 21-day cycles, then 1.3 mg/m2 on days 1, 8, 15, and 22 for three 35-day cyclesCitation11. However, since BORT utilization is most commonly billed and reimbursed in full single-use-vial quantitiesCitation25, the treatment-day dose was assumed to be one 3.5 mg single-use vial.
The drug cost for BORT was based on average sales price (ASP) plus 6% (ASP + 6, 4Q2011), as published by the Centers for Medicare & Medicaid ServicesCitation26: $1450.75 US dollars (USD) per treatment day. The drug cost per treatment day for LEN was based on the average wholesale price (AWP) of $428.18/day minus 16% (AWP−16%, 4Q2011), which is a pharmacy reimbursement rate frequently used by health plansCitation27. Because DEX is available generically, the cost was considered negligible and not included. The base case for the model did not include any patient cost-sharing (i.e., copay, coinsurance) for either treatment regimen, in order to separate the effects of varying benefit designs.
Model inputs: AEs and medical resource utilization
The total medical and AE management costs associated with LEN/DEX or BORT were based partly on methodology from a prior economic model that evaluated medical costs associated with LEN/DEX vs BORTCitation17. The cost calculation included major and common AEs. The AE rate was obtained from the respective prescribing information; event costs were obtained from published fee schedules and literatureCitation17,Citation23,Citation24 ( and ). The AE costs were calculated by multiplying the AE incidence rate by the cost per event. AE event costs were inflated to 2011 USD based on the US medical care services inflation rateCitation28.
Table 1. Adverse event rates, event costs and AE management costs.
Table 2. Medical costs and drug costs.
Medical resource utilization included evaluation and management for MM (office visits), drug administration, hydration, and laboratory testsCitation12,Citation17 during the analysis period until point of relapse. Direct costs for these services were obtained from published Medicare reimbursement rates for the associated procedural codes. In addition, the model included the cost of prophylaxis for deep vein thrombosis (DVT)/pulmonary embolism (PE) in LEN/DEX-treated patients and herpes zoster reactivation in BORT-treated patients. Although not required in the original trials, this prophylaxis is consistent with current medical practice and guidelinesCitation2. Consistent with the previous analysis, the model assumed that 25% and 75% of LEN-treated patients would receive prophylaxis with enoxaparin and aspirin, respectively, for a 75% reduction in the DVT/PE incidence rate (from 11.5% to 2.9%)Citation17. Similarly, all BORT patients were assumed to receive prophylaxis with acyclovir. Cost of progression was included at time of relapse, based on the literatureCitation29.
In the previous analysis, median durations of treatment and cost were determined to be 44 weeks with LEN/DEX and 18 weeks with BORTCitation17. In the current model, medical costs were modeled for protocol-based treatment up to the point of progression, then divided by the number of days in the evaluated time period to derive an average medical cost per day on therapy. The time period in the base-case scenario for both regimens was 12 months.
Time to progression
TTP was the primary end-point for the MM-009/010 and APEX trials. For all trials, TTP was defined as the time between initial patient randomization and the assessment date when signs of progression were first noted. In APEX, median TTP was 6.2 months in patients who received BORTCitation10,Citation11. Composite data from MM-009/010 showed that LEN/DEX resulted in a median TTP of 13.4 monthsCitation7,Citation8,Citation10,Citation11,Citation13. In this model, TTP determined the point at which patients could either receive re-treatment or a change in therapy. In line with NCCN recommendationsCitation2,Citation30, patients were assumed to be re-treated with the same therapy at progression or relapse that occurred after 6 months of therapy.
Model outcomes
The primary outcome was the total cost difference per day between LEN/DEX and BORT.
Sensitivity analysis
A univariate sensitivity analysis was conducted to determine parameters with the most influence on the total cost difference between LEN/DEX and BORT. Alternative scenarios were also tested:
Post-progression treatment: After relapse, patients initially treated with BORT were switched to LEN/DEX vs undergoing BORT re-treatment;
Adding patient cost-sharing;
Alternative physician reimbursement schedules;
Addition of grade 2 peripheral neuropathy (PN) as AE;
Lower administration costs of subcutaneous administration of BORT;
Administration of less than full-vial quantities of BORT; and
Adjusting the actual TTP by a ratio to equate the comparator arm results of the respective trials.
Results
Total costs
The total treatment costs associated with LEN/DEX or BORT over a 12-month period included average daily drug costs, medical services, and AE management. As shown in , the total costs were consistently higher for BORT vs LEN/DEX throughout the 12-month period. The average total cost per day was ∼$47 lower for LEN/DEX vs BORT ($285/day and $332/day, respectively). Over the 12-month period, BORT costs totaled ∼$17,000/year/patient more than for LEN/DEX, with the difference primarily driven by excess medical-care costs with BORT ().
Figure 1. Cumulative total cost difference (BORT minus LEN/DEX) (USD). Excess costs principally due to higher medical and AE management costs for BORT (BORT, bortezomib; DEX, dexamethasone; LEN, lenalidomide).
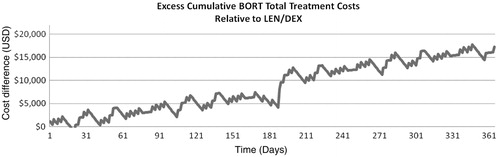
Table 3. Total costs of treatment over a 12-month perioda.
Component costs comparison
Component costs for each treatment are shown in . Before any patient cost-sharing, the average drug cost per day was virtually identical between LEN/DEX and BORT regimens throughout the 1-year period, with a daily difference of under $10/day (similar results were observed when patient cost-sharing was added). The total annual medical costs were 5 times higher for BORT-treated patients than LEN/DEX-treated patients. Average daily AE management costs for BORT and for LEN/DEX were each under $10/day.
Cost per month without progression
An analysis was also conducted to evaluate treatment value for the cost per result obtained over a specific time period (cost per outcome)—in this case, cost per treatment regimen while under an average month of disease control. Distinct from TTP, these costs per month without progression were not determined by a patient reaching a clinical end-point, but were based solely on costs incurred in a month of typical disease management during which disease control had been maintained. For this analysis, the denominator was the cumulative number of days without disease progression, while the numerator was the treatment cost during that period. Whereas cost to progression is most effectively used as a comparator when one regimen does not have a materially longer TTP, in this case, a cost-per-month calculation was considered appropriate, as it removed the biases associated with mismatched treatment durations.
This analysis found that BORT and LEN/DEX were associated with drug and medical costs of $10,105/month and $8949/month, respectively, without progression. BORT had a total monthly cost that was $1155 higher than LEN/DEX, or ∼11% more, per month without progression ().
Sensitivity analysis
A univariate sensitivity analysis indicated that the model inputs with the greatest impact on the cost per day were drug acquisition costs and the daily medical cost for BORT patients. Similar variations in LEN/DEX medical costs, either regimen’s AE management costs, and incorporating patient cost-sharing had minimal impact on the model results.
Alternative scenarios
In addition to the variables evaluated in the univariate sensitivity analysis, alternative scenarios were also tested. To evaluate alternative post-progression treatment, patients initiated on BORT were modeled to switch to LEN/DEX after relapse (median TTP: 6.2 months) (an alternative post-progression treatment regimen was not tested for patients initially treated with LEN/DEX since the 13.4-month median TTP exceeded the 12-month study evaluation period). Because patients in both arms of this scenario are treated with LEN/DEX during the final 5.8 months after progression on BORT, the costs for that period are identical for both arms. Thus, the annual cost difference of $10,549 in favor of LEN/DEX reflects only the excess total treatment cost of BORT during the first 6.2 months before progression, plus the cost of progression. Another sensitivity analysis adjusted the TTP for each regimen based on the ratio of TTP months gained relative to each study’s control arm, raising BORT TTP to 7.4 months and reducing LEN/DEX TTP to 12.1 months; this lowered the annual cost difference to $14,234 in favor of LEN/DEX. A sensitivity analysis involving the inclusion of grade 2 PN (which occurred at a rate of 18% and comprised 51% of all-grade PN cases in the BORT arm of the APEX trial)Citation11 resulted in an additional $354/patient/year in excess costs for BORT. An alternative scenario with a reduction in PN with BORT (as suggested in studies with a healthcare professional-delivered subcutaneous route of administration for BORT)Citation31 yielded minimal changes to the total cost, while another scenario using subcutaneous administrations of BORT (reducing BORT administration costs by $34 per administration) reduced BORT annual costs by $2709. A sensitivity analysis assuming zero waste in a typical administration of BORT in 10% of patients resulted in a $3689 annual reduction in BORT costs; however, full-vial quantity usage (and 37% waste per average patient) may be more representative of standard practice in the US, as evidenced by results at one large US payerCitation25. Other sensitivity analyses (e.g., equal cost-sharing for both products, setting higher cost-sharing for LEN/DEX to be more reflective of the levels applied for oral drugs compared to office-administered products, and raising physician reimbursement for administration to a higher level more representative of commercial health plans) were also conducted. Each analysis further raised the excess total treatment costs of BORT relative to LEN/DEX. Results of these and other alternative scenarios tested are shown in .
Table 4. Sensitivity analyses tested: impact vs base-case cost; cost difference of sensitivity case.
Discussion
Although new treatment options have led to improvements in OS in recent years, the goal of MM treatment continues to be to relieve disease symptoms, maintain remission, avoid complications arising from therapy, and extend patient survivalCitation2. With the advent of newer therapies, survival post-relapse or -refractory disease has increased (median: 30.9 vs 14.8 months for patients not treated with LEN, BORT, or thalidomide)Citation32. As a result, a substantial portion of disease costs, resource use, and time occurs in the context of relapsed/refractory disease. This provides a clear rationale for identifying and comparing treatment costs specific to rrMMCitation21. As such, it is important to consider the total cost burden associated with MM treatment, including drug utilization, medical/diagnostic procedures, lab tests, and administration costsCitation33,Citation34.
This analysis showed that, when evaluating common disease duration, the annual drug costs for rrMM patients were comparable for LEN/DEX and BORT (<$10/day difference). From a health plan perspective in evaluating a relatively low-prevalence hematological cancer, this cost difference is negligible. When the additional costs of associated medical resource utilization and AE management are considered, however, the disparity becomes more meaningful, since the total costs are lower with LEN/DEX vs BORT.
Overall, total drug and medical costs associated with BORT over a 12-month period are >$17,000 higher than those for LEN/DEX. As shown in the sensitivity analysis, regardless of whether patients progressing on BORT therapy are re-treated with BORT or subsequently switched to LEN/DEX, the total costs of rrMM patients initiated on BORT treatment still exceeded those of patients initiated on LEN/DEX, driven principally by higher medical service utilization for BORT, including drug administration costs, office visits, and laboratory tests. In addition, in a sub-analysis comparing cost per outcome, the cost per month without progression was 11% higher for BORT vs LEN/DEX.
LEN/DEX has meaningful cost benefits compared to BORT from a health plan’s perspective. The advantage for LEN/DEX remained, even after considering patient cost-sharing. Despite the fact that cost-sharing is likely to disadvantage LEN/DEX (as many commercial benefit designs do not require coinsurance on physician-administered drugs such as BORT), the total costs for LEN/DEX remained lower. The results of the sensitivity analysis also indicated that changes to the costs of AEs and medical management, the inclusion of BORT-induced grade 2 PN, minor cost reductions from subcutaneous administration of BORT, adjusting TTPs to align comparator arms, adjustments to the amount of BORT vial wastage, or reduction of grade 3/4 BORT-induced PN did not have a substantial impact on the model outcomes.
A strength of the model lies in the equitable comparison of LEN/DEX and BORT in the context of disease progression. In contrast, the model by Fullerton et al.Citation17 compared total costs for each regimen based on the duration of TTP from clinical trials (BORT, 18 weeks; LEN/DEX, 44 weeks)Citation10. However, that inappropriately under-stated the cost of BORT, since patients require continued treatment upon progression. Furthermore, that approach omits recognition of the clinical impact associated with earlier-relapsing patients. Given that LEN/DEX is associated with a longer TTP with ongoing treatment, whereas BORT provides a shorter treatment benefit, that type of cost analysis makes the longer time to disease progression appear to be an economic liability vs a clinical benefit. By evaluating a common treatment period (12 months) for each of LEN/DEX and BORT in rrMM, our modeling approach provides a relevant, equitable basis for evaluating potential real-world costs to a health plan.
Several limitations to the analysis must be noted. Because head-to-head trials of currently recommended MM treatments are not available, indirect comparisons are currently the only evaluation option. Fortunately, because the pivotal trials for both therapies used the same comparator, included similar patient populations, and evaluated the same primary end-point, a high-level comparison could reasonably be undertakenCitation11,Citation13,Citation14. However, patient cross-over that occurred in the trials may confound the results. Furthermore, the BORT registrational studies were conducted as monotherapy without DEX; a potential additional TTP benefit of off-label BORT use with DEX has not been quantified in registrational trials. Second, modeling requires a variety of assumptions regarding the disease, treatment patterns, and costs; the results presented represent an estimate of the cost per-patient per-year of LEN/DEX and BORT to treat rrMM. For example, patient cost-sharing may vary across health plans, which would impact the actual drug costs to the plan. Despite efforts to identify and quantify all components that may contribute substantially to total costs in rrMM treatment, some costs may have been overlooked. Literature-based estimates of AE management may not reflect current costs or standards of care; however, AE management costs did not represent a material percentage of the overall cost of care. Detailed sensitivity analyses were undertaken to evaluate uncertainty in the model assumptions and variables.
Furthermore, actual treatment patterns post-relapse may vary from the scenario modeled. Physicians may not always begin new therapy upon relapse, or there may be additional costs associated with progression or post-progression treatment that were not reflected in this analysis. As such, management costs for a patient before and after disease relapse may differ. Because BORT-treated patients in this model had a relapse prior to the completion of the 12-month period (median TTP 189 days), the medical and AE management costs incurred for treatment following relapse may be higher or lower than those incurred prior to relapse, regardless of choice of subsequent therapy.
Although the 12-month time frame is useful to compare the treatment regimens, since it reflects a common time frame of interest to US payers and captures the bulk of the duration of treatment for rrMM from initiation to relapse, it does not capture the entirety of clinical benefit received or costs incurred from either treatmentCitation30,Citation33,Citation34. At this time the evidence in the literature is not conclusive regarding whether extended TTP in rrMM translates into extended OS. If it does not, then the cost differences identified here would be the same as for a lifetime analysis, since the subsequent costs and time periods would be equal (potentially up to a median of another 3 years, based on recent trends in OS for the disease and a likely 2-year or longer treatment period prior to the year of relapse treatment modeled here). Alternatively, if extended progression-free survival was to partly or completely result in extended OS, then LEN/DEX would potentially result in up to an additional 7 months of lifetime cost and OS gain; this gain would have per-month costs likely to be more similar to the costs measured here as opposed to the end-of-life costs, i.e., ∼$8000 per month and per month of OS gained. Further studies are needed to evaluate lifetime costs. Nevertheless, the preponderance of BORT costs associated with drug, administration, and AE management, as shown in the model, suggests that these or other factors are unlikely to qualitatively affect the end result.
In summary, this analysis showed that, while the treatments had comparable drug costs, ongoing medical and AE management costs associated with BORT were substantially higher (by $17,136 annually) vs LEN/DEX for the 12-month period. The cost difference favored LEN/DEX throughout the 12-month period and across all sensitivity analyses, as well as in the cost per outcome. Evaluations such as this, which compare all medical and drug costs for specific treatments over a common time frame, using approved treatment regimens and a widely accepted outcome measure (TTP), provide a transparent and accurate perspective for comparison. These results may be generalizable to real-world patient-treatment patterns, and should provide substantial utility for payer decision-making.
Transparency
Declaration of funding
This research was funded by Celgene Corporation.
Declaration of financial/other interests
BD has disclosed that he is a consultant to Celgene Corporation, Millennium Pharmaceuticals, Onyx Pharmaceuticals, and Novartis. GB, ZK, and MH have disclosed that they are employees of Celgene Corporation. CP has disclosed that he is an employee of United BioSource Corporation. IB has disclosed that he is a consultant to Celgene Corporation. Contributions: Conception and Design: BD, GB, ZK, MH; Collection & Assembly of Data: BD, GB; Data Analysis and Interpretation: All; Manuscript Writing and Approval: All. JME Peer Reviewers on this manuscript have no relevant financial relationships to disclose.
Acknowledgments
The authors would like to acknowledge Evelyn Sarnes and others from Xcenda, LLC, for their assistance in preparing the manuscript. Previous presentation: An earlier version of the analysis was the subject of an abstract and poster at the most recent International Myeloma Workshop in 2011.
References
- Anderson KC, Kyle RA, Rajkumar SV, et al. Clinically relevant end points and new drug approvals for myeloma. Leukemia 2008;22:231-9
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: multiple myeloma. Version 1.2012. National Comprehensive Cancer Network, Fort Washington, PA. 2012. http://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf. Accessed 15 October 2012
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011;364:1046-60
- Barlogie B, Tricot G. Complete response in myeloma: a Trojan horse? Blood 2006;108:2134
- Kane RC, Bross PF, Farrell AT, et al. Velcade: U.S. FDA approval for the treatment of multiple myeloma progressing on prior therapy. Oncologist 2003;8:508-13
- Durie BGM. Role of new treatment approaches in defining treatment goals in multiple myeloma – the ultimate goal is extended survival. Cancer Treat Rev 2010;36(Suppl 2):S18-23
- National Center for Biotechnology Information (NCBI). Multiple Myeloma. U.S. National Library of Medicine, Bethesda, MD. 2011. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001609/. Accessed 15 October 2012
- Dimopoulos MA, Chen C, Spencer A, et al. Long-term follow-up on overall survival from the MM-009 and MM-010 phase III trials of lenalidomide plus dexamethasone in patients with relapsed or refractory multiple myeloma. Leukemia 2009;23:2147-52
- Kastritis E, Anagnostopoulos A, Roussou M, et al. Reversibility of renal failure in newly diagnosed multiple myeloma patients treated with high-dose dexamethasone-containing regimens and the impact of novel agents. Haematologica 2007;92:546-9
- Richardson PG, Sonneveld P, Schuster M, et al. Extended follow-up of a phase 3 trial in relapsed multiple myeloma: final time-to-event results of the APEX trial. Blood 2007;110:3557-60
- Richardson PG, Sonneveld P, Schuster MW, et al. Bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med 2005;352:2487-98
- Stadtmauer EA, Weber DM, Nieszvizky R, et al. Comparison of lenalidomide plus dexamethasone therapy used at first relapse versus later salvage therapy in relapsed or refractory multiple myeloma patients. J Clin Oncol 2009;27(15S): abstract 8594
- Weber DM, Chen C, Niesvizky R, et al. Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med 2007;357:2133-42
- Dimopoulos M, Spencer A, Attal M, et al. Lenalidomide plus dexamethasone for relapsed or refractory multiple myeloma. N Engl J Med 2007;357:2123-32
- Kenney J. Advances in the management of multiple myeloma: implications for payers. Am Health Drug Benefits 2011;4(2 Suppl 4):S59-60
- Messori A, Maratea D, Nozzoli C, et al. The role of bortezomib, thalidomide and lenalidomide in the management of multiple myeloma: an overview of clinical and economic information. Pharmacoeconomics 2011;29:269-85
- Fullerton D, Huleatt H, Marantz J, et al. Treatment of relapsed myeloma: a budget impact model comparing single agent bortezomib with combination lenalidomide and high-dose dexamethasone. Presented at the Academy of Managed Care Pharmacy 2007 Educational Conference, Boston, MA, October 24-27, 2007
- Moeremans K, Annemans L. An update: health economics of managing multiple myeloma. Eur J Cancer 2006;42):1684-91
- Gaultney JG, Redekop WK, Sonneveld P, et al. Critical review of economic evaluations in multiple myeloma: an overview of the economic evidence and quality of the methodology. Eur J Cancer 2011;47:1458-67
- Durie BG, Borrello I, Binder G, et al. Treatment cost comparison in relapsed multiple myeloma. Presented at the 13th International Myeloma Workshop, Paris, France, May 3-6, 2011
- Cook R. Economic and clinical impact of multiple myeloma to managed care. J Manag Care Pharm 2008;14(7 Suppl):19-25
- Schey S, Higginson I. Cost-effectiveness of lenalidomide in multiple myeloma. Expert Rev Pharmacoecon Outcomes Res 2010;10:229-38
- REVLIMID [prescribing information]. Summit, NJ: Celgene Corporation, 2010
- Velcade [prescribing information]. Cambridge, MA: Millennium Pharmaceuticals, 2010
- Binder G, Harwin W, Stemkowski S, et al. Drug resource use and costs for novel agents in multiple myeloma. J Clin Oncol 2012;30(Suppl 15):abstract e18560
- Centers for Medicare & Medicaid Services. Payment allowance limits for Medicare part B drugs. CMS, Bethesda, MD. 2010. http://www.cms.gov/apps/ama/license.asp?file=/McrPartBDrugAvgSalesPrice/downloads/October_2010_ASP_Pricing_File.zip. Accessed 15 October 2012
- Curtiss FR, Lettrich P, Fairman KA. What is the price benchmark to replace average wholesale price (AWP)? J Manag Care Pharm 2010;16:492-501
- US Bureau of Labor Statistics. Consumer Price Index, All Urban Consumers. US Bureau of Labor Statistics, Washington, DC. 2012. http://data.bls.gov/cgi-bin/surveymost?cu. Accessed 15 October 2012
- Wang S, Huang H, Ba-mancini A, et al. The cost-effectiveness of bortezomib plus melphalan and prednisone versus lenalidomide plus melphalan and prednisone with continuous lenalidomide maintenance treatment for the initial treatment of multiple myeloma in the USA, poster, ISPOR May 2011, Baltimore, MD
- Rajkumar SV. Multiple myeloma: 2011 update on diagnosis, risk-stratification, and management. Am J Hematol 2011;86:57-65
- Moreau P, Pylypenko H, Grosicki S, et al. Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma: a randomised, phase 3, non-inferiority study. Lancet Oncol 2011;12:431-40
- Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood 2008;111:2516-20
- Armoiry X, Fagnani F, Benboubker L, et al. Management of relapsed or refractory multiple myeloma in French hospitals and estimation of associated direct costs: a multi-centre retrospective cohort study. J Clin Pharm Ther 2011;36:19-26
- Koleva D, Cortelazzo S, Toldo C, et al. Healthcare costs of multiple myeloma: an Italian study. Eur J Cancer Care (Engl) 2011;20:330-6
- Goulart B, Ramsey S. A trial-based assessment of the cost-utility of bevacizumab and chemotherapy versus chemotherapy alone for advanced non-small cell lung cancer. Value Health 2011;14:836
- Calhoun EA, Chiang C-H, Welshman EE, et al. Evaluating the total costs of chemotherapy-induced toxicity: results from a pilot study with ovarian cancer patients. Oncologist 2001;6:441-5
- Elting LS, Escalante CP, Cooksley C, et al. Outcomes and cost of deep venous thrombosis among patients with cancer. Arch Intern Med 2004;164:1653-61
- Dranitsaris G, Maroun J, Shah A. Severe chemotherapy-induced diarrhea in patients with colorectal cancer: a cost of illness analysis. Support Care Cancer 2005;13:318-24
- Tina Shih YC, Xu Y, Elting LS. Costs of uncontrolled chemotherapy-induced nausea and vomiting among working-age cancer patients receiving highly or moderately emetogenic chemotherapy. Cancer 2007;110:678-85
- White RR, Lenhart G, Singhal PK, et al. Incremental 1-year medical resource utilization and costs for patients with herpes zoster from a set of US health plans. Pharmacoeconomics 2009;27:781-92
- Eber M, Laxminarayan R, Perencevich E, et al. Clinical and economic outcomes attributable to health care–associated sepsis and pneumonia. Arch Intern Med 2010;170:347-53
- Vickrey E, Allen S, Mehta J, et al. Acyclovir to prevent reactivation of varicella zoster virus (herpes zoster) in multiple myeloma patients receiving bortezomib therapy. Cancer 2009;115:229-32
- Micromedex 2.0: RedBook Online. 2011: http://www.micromedex.com/index.html. Accessed 15 October 2012
- Physician’s Fee and Coding Guide. Duluth, GA: Mag Mutual, 2011
- Centers for Medicare & Medicaid Services. Hospital Outpatient PPS Addendum A. Centers for Medicare & Medicaid Services, Baltimore, MD, 2011. http://www.cms.gov/HospitalOutpatientPPS/AU/. Accessed 15 October 2012
- US Bureau of Labor Statistics. CPI Detailed Report - Data for October 2010. US Bureau of Labor Statistics, Washington, DC. 2010. http://www.bls.gov/cpi/cpid1010.pdf. Accessed 15 October 2012
Notice of correction
Since original online publication, a correction has been made to Table 2. The value for ‘Number of office visits’ in the column ‘LEN/DEX’ has been changed from 6 to 16. The current version includes this correction and matches the printed issue.