Abstract
Many aspects of human physiology and behavior are dominated by 24-hour circadian rhythms that have a major impact on our health and well-being, including the sleep-wake cycle, alertness and performance patterns, and many daily hormone profiles. These rhythms are spontaneously generated by an internal “pacemaker” in the hypothalamus, and daily light exposure to the eyes is required to keep these circadian rhythms synchronized both internally and with the external environment Sighted individuals take this daily synchronization process for granted, although they experience some of the consequences of circadian desynchrony when “jetlagged” or working night shifts. Most blind people with no perception of light, however, experience continual circadian desynchrony through a failure of light information to reach the hypothalamic circadian clock, resulting in cyclical episodes of poor sleep and daytime dysfunction. Daily melatonin administration, which provides a replacement synchronizing daily “time cue,” is a promising therapeutic strategy, although optimal treatment dose and timing remain to be determined.
Muchos aspectos fisiológicos y conductuales del ser humano están controlados por ritmos circadianos de 24 horas, los que tienen un gran impacto en nuestra salud y bienestar Estos ritmos incluyen el ciclo sueño-vigilia, el alerta y los patrones de varias funciones, como también el perfil de secreción diaria de muchas hormonas. Estos ritmos se generan espontáneamente por un “marcapaso” interno en el hipotálamo y se requiere de la exposición de los ojos a la luz diurna para mantener estos ritmos circadianos sincronizados tanto internamente como con el ambiente externo. Los sujetos videntes tienen este proceso de sincronización asegurado, aunque ellos experimenten algunas de las consecuencias derivadas de la falta de sincronía cuando tienen un “jetlag” o trabajan en turnos nocturnos. La mayoría de las personas ciegas no percibe la luz; sin embargo, experimentan continuas faltas de sincronía circadiana debido a que falla la llegada de la información luminosa al reloj circadiano hipotalámico, lo que se traduce en episodios cíclicos de mal dormir y mal funcionamiento durante el día. La administración diaria de melatonina proporciona un sustituto para la sincronización diaria de la “clave temporal”, y aunque constituye una estrategia terapéutica promisoria, aun falta determinar el momento más adecuado de la administración y la dosis terapéutica óptima.
De nombreux aspects de la physiologie et du comportement humain sont dominés par les rythmes circadiens de 24 h qui ont un impact majeur sur notre santé et notre bien-être, notamment le cycle veille-sommeil, les variations quotidiennes des processus attentionnels et de performance, et la sécrétion de nombreuses hormones. Ces rythmes circadiens sont générés spontanément par un « pacemaker » interne situé dans l'hypothalamus. Une exposition quotidienne des yeux à la lumière est nécessaire pour conserver la synchronisation de ces rythmes à la fois entre eux et avec l'environnement externe. Les voyants considèrent cette synchronisation quotidienne comme évidente, tout en expérimentant certaines conséquences de la désynchronisation circadienne en cas de décalage horaire ou de travail en horaire posté. La plupart des aveugles, n'ayant aucune perception de lumière, subissent une désynchronisation circadienne permanente par impossibilité de l'information lumineuse d'atteindre l'horloge circadienne hypothalamique. Ceci conduit à des épisodes cycliques de mauvais sommeil et de mauvais fonctionnement diurne. En resynchronisant les plages horaires chaque jour, l'administration quotidienne de mélatonine est une stratégie thérapeutique prometteuse, bien qu'il faille encore en préciser l'horaire d'administration et la posologie optimale.
Many aspects of human physiology and behavior are dominated by 24-hour rhythms that have a major impact on our health and well-being. For example, sleep-wake cycles, alertness and performance patterns, core body temperature rhythms, and the production of hormones such as melatonin and Cortisol are all regulated by an endogenous near-24-hour oscillator in the suprachi-asmatic nuclei (SCN) of the anterior hypothalamus. The cells in these nuclei spontaneously generate rhythms with a period close to, but not exactly, 24 hours, and in order for the circadian pacemaker to ensure that physiology and behavior are appropriately timed to anticipate events in the outside world, environmental time cues must be able to reset this internal clock to 24 hours. The major environmental time cue that resets these rhythms in mammals is the 24-hour light-dark cycle generated by the earth's axial rotation. Light information is captured exclusively by the eyes using specialized retinal photoreceptors and transduced directly to the SCN via a dedicated neural pathway, the retinohypothalamic tract (RHT). Each day the light-dark cycle resets the internal clock, which in turn synchronizes the physiology and behavior controlled by the clock.
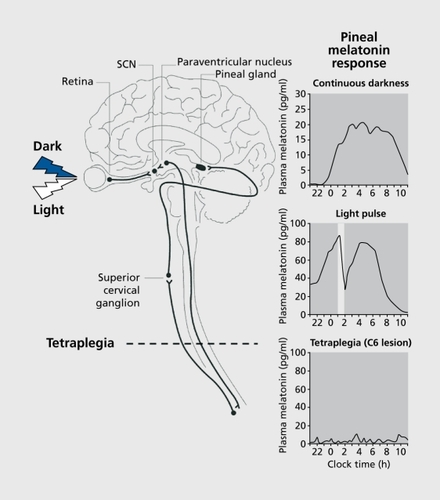
The major biochemical correlate of the lightdark cycle is provided by the pineal melatonin rhythm. Under normal light-dark conditions, melatonin is produced only during the night, and provides an internal representation of the environmental photoperiod, specifically nightlength. The synthesis and timing of melatonin production requires an afferent signal from the SCN which projects to the pineal gland via the paraventricular nucleus and the superior cervical ganglion. Light exposure during the night also inhibits melatonin production acutely and provides an indirect assessment of light input to the SCN via the RHT ().Citation1-Citation4 Given the close temporal relationship between the SCN and melatonin production, the melatonin rhythm is often used as a marker of circadian phase and the melatonin suppression response as a proxy for RHT-SCN-pineal integrity and sensitivity
The role of light in circadian entrainment
Under normal conditions, the vital importance of daily light-dark exposure to entrain circadian rhythms is taken for granted. For example, although not consciously perceived, the ability to sleep at night and be awake in the day is largely controlled by the circadian system, which promotes sleep during the night and wakefulness during the day via alterations in efferent signals from the SCN to other hypothalamic areas controlling sleep-wake states.Citation5 The difficulties associated with trying to sleep during the day or be awake at night at the “wrong” circadian time is readily observed in sighted people following rapid transmeridian travel (“jet lag”)Citation6 or in night-shift workers.Citation7 When traveling across multiple time zones, or when changing from a day to a night shift, the change in the timing of the light-dark exposure is too rapid for the internal circadian pacemaker to synchronize to immediately A 12-hour shift in sleep timing or time zone may take as long as 2 weeks to become resynchronized to,Citation8 and often shift times or the time zone are changed again before adaptation has occurred. Consequently, the individual's sleep pattern becomes desynchronized from the circadian system and, in the case of shift workers, daytime sleep duration is short, sleep efficiency is poor, and night-time waking alertness and performance are impaired,Citation9 accounting for the high incidence of accidents and injuries experienced by nightshift workers.Citation10 Other functions also become desynchronized under such conditions, for example, postprandial metabolism. When meals are taken during the biological night, they cannot be metabolized as efficiently as when eaten during the day, and consequently postprandial levels of glucose, Insulin, and fats are elevated.Citation11-Citation13 In the long term, the regular Impairment of metabolism Induced over years of shiftwork may lead to chronically elevated clrculating levels of Insulin and fat, and may increase the risk of developing Insulin resistance, diabetes, or cardiovascular disease.Citation14 Gastrointestinal discomfort is also a common complaint In jet lag,Citation15 most likely due to the temporal misalignment of circadian oscillators In peripheral tissues (eg, the liver, kidney, esophagus, and stomach) that have recently been Identified (for review see ref 16).
The potential Importance of light In human circadian entrainment was first explored in cave experiments, where investigators measured rhythms In physiology and behavior when shielded from the solar day (although dim artificial light was generally available).Citation17,Citation18 These studies Indicated that the circadian pacemaker did not oscillate exactly on a 24-hour day, but had a circadian period (x) that was on average slightly longer than 24 hours. Studies of subjects kept in temporal Isolation,Citation19 In dim Hght-dark cycles,Citation20,Citation21 or on very long (eg, 28-h, 30-h, 42.85 h) or very short (eg, 11-h, 20-h) day-lengths outside the range of entrainment of the biological clock have also shown that the period of the circadian clock Is not exactly 24 hours In humans (average -24.2 h)Citation22,Citation23 similarly to that In other mammals. Under such nonentrained conditions, the rhythms controlled by the circadian system ”free-run“ at the endogenous period of the biological clock. For example, If a person's nonentrained period Is 24.5 h, the sleep-wake cycle and other rhythms will also cycle with a period of 24.5 h and the subject will therefore go to sleep 0.5 hours later each day, when measured using the 24hour clock (see below).
Real-world environments where altered llght-dark exposure can result In circadian desynchrony in sighted individuals Include submarines, where the dim light levels and rapidly rotating duty cycles cause the circadian system to “free-run” with a non-24-hour cycleCitation24; during spaceflight, where unusual light-dark exposure, combined with imposed non-24-hour “workdays,” cause disruption to circadian rhythms and sleepCitation25,Citation26; and during polar winters where, In the absence of any environmental lightdark cycle, Inadequate or poorly timed artificial light exposure can fail to entrain circadian rhythms in sleep, performance, and metabolism.Citation27-Citation29 Although the light-dark cycle Is the primary environmental time cue, ”nonphotlc“ time cues, such as sleep, exercise, food, and some drugs, are also able to reset the circadian pacemaker (for review see ref 30), and are potentially Important for blind patients (see below).
The effect of visual impairment on circadian entrainment
Early studies of hormone rhythm disorders in the blind
If ocular light exposure Is the most Important environmental circadian synchronizer, the obvious question is, what happens to the circadian rhythms In visually Impaired people? Abnormal hormonal patterns have been reported in some visually Impaired patients for more than five decades. In the 1940s, Remler recognized that some blind patients had normal 24-hour rhythms whereas some had Inverted rhythms In rectal temperature, heart rate, blood pressure, and urinary excretion (1948Citation31 cited In Hollwich and DleckhuesCitation32). Subsequently, Orth and Island,Citation33 Kreiger and Rizzo,Citation34 Bodenheimer et al,Citation35 and D'Allessandro et alCitation36 all found Irregularities In the plasma profiles of corticosteroid production In a majority of blind subjects. Orth and IslandCitation33 studied three subjects with no conscious perception of light (NPL) and demonstrated a normal, an abnormal, and a free-running rhythm of 17-hydroxycorticosterold (17-OHCS) production In these subjects. Kreiger and RizzoCitation34 showed that five out of seven blind subjects with light perception (LP) and nine of 12 NPL subjects had abnormal ll-hydroxy corticosteroid (11-OHCS) rhythms. Similarly, Bodenheimer et alCitation35 reported that grouped data of 24-h Cortisol measurements from seven NPL subjects showed a phase difference compared with sighted controls. D'Allessandro et alCitation36 presented mean plasma Cortisol data from 11 NPL patients that did not show 24-h rhythmiclty. All the studies emphasized the Importance of light In modulating the secretion of corticosteroids and noted a split of these rhythms from the sleep-wake cycle. Similarly, Irregularities of sleep and its timing were related to an abnormal phase of rectal ternperature.Citation37,Citation38 The rhythm of excretion rates of electrolytes (Na+, Cl-, K+) was also shown to be abnormally timed with a reduced amplitude In the blind.Citation39,Citation40
Several early studies did not find any Irregularities in the rhythms of blind individuals, however. Mlgeon et alCitation41 failed to find any differences In the diurnal pattern of plasma and urinary excretion of 17-OHCS between sighted subjects, night workers, and blind subjects with no conscious light perception (NPL), although a reduction In the amplitude of plasma 17-OHCS was observed In the blind people. Weltzman et alCitation42 found normal Cortisol and growth hormone rhythms In seven NPL subjects comparable to sighted Individuals. Similarly, Scheving et alCitation43 found no phase difference in the epinephrine and norepinephrine rhythms of 14 blind subjects compared with sighted subjects, although there was an Increase In the mesor of norepinephrine levels In these subjects.
A large study of the “endocrine system” of several hundred blind Individuals was conducted by Hollwich and Dleckhues.Citation32 They found abnormalities in a wide variety of biochemical measurements In totally blind subjects (n=220) compared with those with severely Impaired vision (n=140) and sighted subjects (n=50). These changes Included reduced serum levels of glucose, protein, Cortisol, sodium, and raised levels of creatinine and potassium which were mirrored In urinary analysis. Unfortunately, samples were taken only once or overnight, and did not take into account any age or circadian phase differences between individuals. They did postulate the existence, however, of an “excitatory effect” of light on the hypothalamus via an “energetic pathway of the optic system, ...independent of the visual pathway” that stimulated “releasing factors” from the hypothalamus that regulated hormone levels, an observation that correctly anticipated confirmation of a physiologically distinct retinohypothalamlc tract. Hollwich and Dleckhues also concluded that the reduction In metabolic activity In the blind accounted for the complaints of blind patients (including diminished physical capacity, Insomnia, autonomic and emotional disturbances, desynchrony, and circadian rhythm sleep disorders). The failure to follow circadian rhythms longitudinally within individuals, however, limited the Interpretation of these early studies.
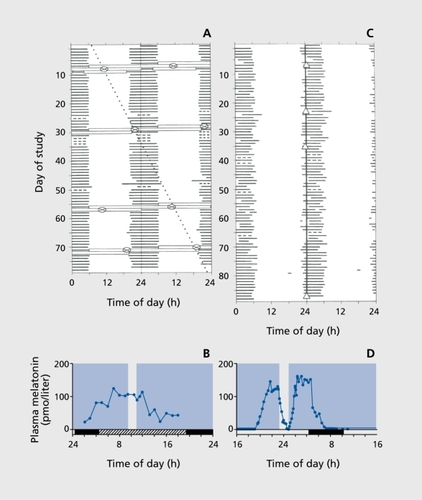
The first report of melatonin rhythms In the blind was made by Smith and colleagues who showed that four blind men had higher day - than night-time melatonin levels,Citation44 the opposite of what would be expected in sighted subjects (Figure 1). Subsequently, Lewy and NewsomeCitation45 Investigated plasma melatonin profiles In 10 blind subjects (9 NPL, 1 LP) and showed that six subjects had an abnormally timed melatonin rhythm, three of these being phase-advanced and three being phase-delayed. Longitudinal follow-up of two of these patients showed one subject with a stable but abnormally entrained melatonin rhythm (peak time 10.00-12.00 h, an approximate delay of 8 hours compared with normal) and the other subject had a free-running melatonin rhythm with a period of 24.7 h.Citation45 The same group later conducted a more extensive longitudinal study of the plasma melatonin rhythms In 20 NPL subjects,Citation46 and confirmed a heterogeneous distribution of melatonin rhythm types. Three subjects had normally phased melatonin rhythms, three were abnormally entrained, and 11 had free-running melatonin rhythms with periods ranging from 23.86 to 25.08 h.Citation46 The remaining three subjects appeared to be arrhythmic.
Early studies of sleep disorders in the bind
Another prediction that can be made If light Is Important for circadian entrainment is that sleep disorders would be more prevalent in blind compared with sighted subjects, or in those without light perception, as compared with those with some degree of light perception. Several epidemiological studies have investigated these hypotheses. Miles and Wilson first reported that 76% of blind subjects with a range of visual loss complained of a sleep-wake disorder (n=50).Citation47 Additionally, 40% of subjects recognized that the symptoms were cyclic or episodic, an important characteristic of circadian rhythm sleep disorders (see below). Sasaki et alCitation48 demonstrated a lower Incidence of sleep-wake complaints (40%) in 73 blind teenagers, although they did postulate that an Increase in sleep disorder (delayed sleep phase syndrome and non-24-h sleepwake rhythm) was associated with a decrease in light perception. More recently, Léger et alCitation49 reported on the results of a postal study In ~ 800 blind Individuals, who were age, sex - and location-matched with sighted controls. Overall, significantly more of the blind Individuals were said to have at least one sleep disorder (83% - at least one of latency, night-time and early-mornlng awakenings, reduced sleep duration or quality) and In addition, 17% of the subjects fulfilled the criteria for diagnosis of free-runnlng sleep patterns.Citation50 Unfortunately, no Information was provided about the severity of visual loss In Individuals with “freerunning” sleep or on any relationship between sleep disorder and visual acuity A slmilar-sized postal study of UK guide-dog owners (n=1139) was also conducted In the UK by Moseley et alCitation51 who reported a low prevalence of subjective disorder overall (18%) which reduced to 14% In subjects who did not report being depressed (n=981).The methodology for sleep assessment was not described, and the authors stated that sleep disorders were likely to be due to other factors than circadian rhythm disorders caused by loss of light perception.
In order to address whether sleep disorders were associated with loss of light perception, we conducted a survey of 388 registered blind Individuals with a range of visual acuities (n=54 with no perception of light [NPL] and n=330 with visual acuity from 20/200 vision to light perception only [LP]).Citation52 Sleep disorders were assessed using the Pittsburgh Sleep Quality Index (PSQI score > 5) and subjects with depressive symptoms were excluded. Disturbance of sleep was recorded In nearly 50% (189/388) of the blind subjects overall. The prevalence was higher (66%) and the sleep disturbance was more severe (mean PSQI ± SD = 8.1 ± 1.1); however, In the NPL group compared with those blind subjects with a visual acuity of LP or better (46%, mean PSQI =5.8 ± 0.4), or sighted controls (9%, mean PSQI =2.9 ± 0.5; n=44).Citation52 These data are consistent with the hypothesis that reduced photic input to the circadian pacemaker may Increase the risk of circadian rhythm sleep disorders.
Circadian rhythm disorders in the blind
The first study to describe conclusively that circadian rhythm disorders per se occurred in the blind was conducted by Miles et al In 1977.Citation53 They showed that a blind man with no conscious perception of light (NPL) had nonentrained “free-running” sleep-wake, temperature, alertness, performance, Cortisol and urinary excretion rhythms with a period (τ) of 24.9 hours when the subject lived freely without restriction. Similarly, Orth et alCitation54 demonstrated a free-running Cortisol rhythm with a period of 24.5 h in a 52-year-old woman with NPL, and other cases reported similar results In sleep and/or hormonal rhythms.Citation55-Citation59 These periodicities persisted despite attempts to entrain the rhythms using a strict regime of bedtime, meals, and activity, or knowledge of clock time. In order to extend these findings, In 1994 we started a series of studies to investigate in more detail the relationship between visual Impairment and circadian rhythm disorders under real-world conditions.Citation60-Citation62 To date, we have studied 67 blind adults (aged 17 to 74 years; 48 males, 19 females) with varying visual acuities using a home-based protocol where subjects are asked to maintain a daily sleep log for at least 4 weeks, and wear an activity monitor continuously.Citation63 For 48 hours per week, most subjects are also asked to rate their alertness and mood every 2 hours while awake using four 9-point Likert scales, and complete a four-choice serial auditory reaction time test after each alertness rating. Finally, they are asked to collect their urine for the same 48 hours In 4-hourly episodes while awake plus an 8-hourly collection overnight, record the volume by weight, and retain a sample for analysis. The urine samples are analyzed for 6-sulphatoxymelatonin (aMT6s) (),Citation64 the major urinary metabolite of melatonin, or Cortisol, which provide a reliable marker of circadian phase.Citation27,Citation64-Citation66
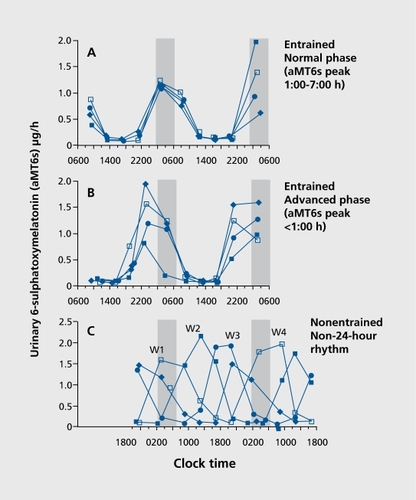
The Incidence of circadian rhythm disorders Is related to the degree of visual acuity. Of the 30 individuals with light perception (LP; 19 males, 11 females), 77% had normally entrained aMT6s rhythms, and four (13%) had abnormally phased rhythms (2 advanced and 2 delayed). Two subjects had no detectable rhythm and one subject with minimal LP In one eye only exhibited a free running aMT6s rhythm (x = 24.62 h). Conversely, the majority of NPL subjects (76%) had abnormal aMT6s rhythms (either abnormally entrained or ”free running“). Of those NPL subjects with at least one eye, 11 (46%) had free running aMT6s rhythms (x range = 23.92-24.79 h), 5 (21%) were abnormally phased (3 advanced, 2 delayed) and 7 (29%) were normally entrained. One subject had no significant rhythm. One subject with small vestigial eyes located under the skin (cryptophthalmos) also had normal aMT6s and Cortisol rhythms. All of the bilaterally enucleated subjects (n=12) exhibited free running rhythms with periods ranging from 24.13 to 24.81 h.
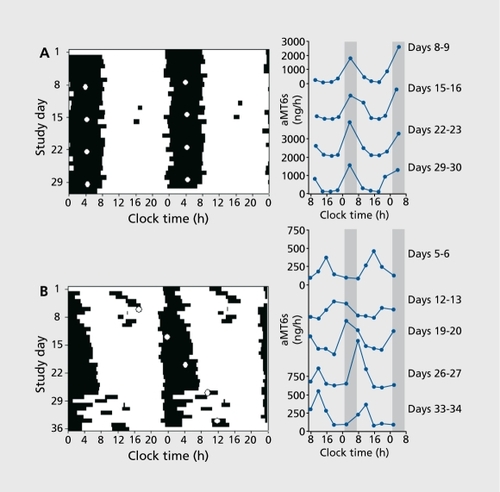
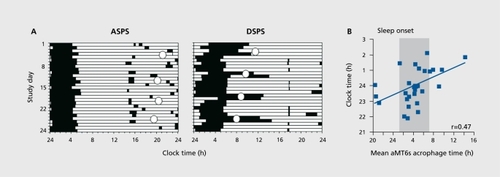
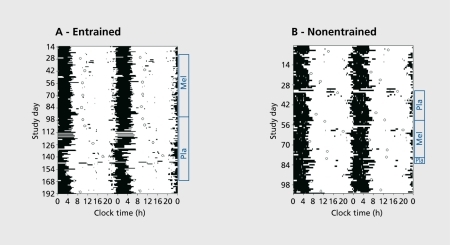
Although abnormal timing of hormonal patterns can confirm the presence of a circadian rhythm disorder, patients complain about the resultant circadian rhythm sleep disorder, and disturbed sleep is the most commonly reported symptom associated with misaligned circadian rhythms (). and ().Citation62,Citation67 Irregularities of sleep and its timing were previously related to an abnormal phase of the rectal temperature rhythmCitation37,Citation38 and in 1990, Martens et al reported that 71% of NPL subjects (n=16) complained of a chronic sleep disorder associated with increased sleep episodes and increased daytime sleep.Citation68 We have extended these findings and showed that sleep depends on clrcadlan phase,Citation69 even under real-world conditions.Citation62 In entrained subjects, the timing of sleep was highly correlated with the timing of the aMT6s rhythm such that subjects with advanced aMT6s rhythms had a relatively earlier sleep time and subjects with delayed aMT6s rhythms had a later sleep time (Figure 4),Citation62 In ”free-running“ subjects, a more complicated pattern emerges where sleep exhibits a non-24-hour pattern that cycles in and out of synchrony with the 24-hour social day on which most subjects try to live (Figure 3B). The episode of poor sleep is characterized by short duration night-time sleep and a high propensity for daytime naps the timing of which coincides with the aMT6s peak as the clrcadlan system drives sleepiness during the biological (but not social) night.Citation62,Citation70 The cyclic sleep-wake pattern, formally termed “non-24-hour sleepwake disorder,”Citation50 persists ad Infinitum and can be extremely disruptive and debilitating, especially In Individuals with periods very close to 24 hours, when sleep can remain misaligned from the clrcadlan cycle for many months.
In addition to affecting sleep, circadian rhythm disorders also Impact waking function. In addition to the high propensity for naps during the day,Citation70 subjects also rate themselves more sleepy and more miserable and perform worst when they are awake at an adverse circadian phase.Citation71 In entrained subjects, the dally profile of sleepiness, mood, and performance depends on the circadian phase of the wake episode, such that advanced subjects feel better In the early part of the day and worse late In the day, whereas delayed subjects report feeling very sleepy for the first half of the day, but then gradually getting better as the day goes on. These alertness and performance profiles are similar to those experienced by extreme “morning” and “evening” types who also sleep and wake at relatively abnormal circadian phases.Citation72 In free running subjects, the rhythms in alertness and performance also free-run, as first shown in the case by Miles et al,Citation53 such that subjects report feeling the worst when awake at the time of peak aMT6s production and best when awake at a normal circadian phase, when no aMT6s is being produced, as occurs in most sighted subjects.
The effect of light in the blind
The effect of visual impairment on circadian photoreception
The impact of different types of visual impairment on the circadian system has been used as an indirect method to assess the photoreceptor systems mediating circadian and other nonvisual responses to light. Firstly, these studies have shown that eyes are required for circadian photoreception; individuals without eyes, either through bilateral enucleation or as a result of developmental disorders, are unable to entrain their circadian pacemaker to the 24-hour light-dark cycle.Citation61 Similarly, the majority of totally blind individuals who retain their eyes but cannot consciously perceive light also exhibit circadian rhythms that are not entrained to the 24-hour light-dark cycle, as described above.
Disorders of the visual system do not always attenuate the circadian effects of light, however, demonstrating a functional separation of the visual and circadian photoreception systems. As outlined previously, the majority of legally blind individuals who retain some degree of light perception, even with very little usable vision in some cases, have normally entrained clrcadlan rhythms.Citation61 Primary loss of the central or peripheral visual fields Is also not associated with circadian rhythm disorders,Citation61,Citation63 suggesting that the circadian photoreceptor system Is less sensitive to the spatial distribution and Intensity of light than vision. Color blindness, a more specific lesion of the threecone photoplc visual system, also does not attenuate circadian responses to light, as measured by acute suppression of pineal melatonin,Citation73 suggesting that the cones are not the primary photoreceptors mediating this response. Finally, and most definitively, It has been demonstrated that a small proportion of blind people without light perception retain normal circadian phase-shifting and melatonin suppression responses to light, even In the absence of any func tlonal rods or cones, as assessed by conscious ability to detect light, visually-evoked potentials, or electroretinogram (). Citation74,Citation75 As expected If their eyes contained fully functional circadian photoreceptors, these Individuals exhibit normally entrained 24-hour rhythms under realworld conditions and do not report sleep disorders.Citation74 The effects of light in these subjects are mediated excluslvely via the eyes as, when their eyes are covered, the effects of light are Inhibited. Thus, circadian photoreception can be maintained In some humans In the absence of a functional visual system, as has also been shown in transgenic and developmental rodent models of blindness (for review see ref 76). While intact circadian photoreception explains the normally entrained 24-hour rhythms in about 20% of entrained NPL subjects, most blind people who exhibit 24-hour rhythms are not affected by light (Citation63, Lockley et al, unpublished results) and are either entrained by nonphotic time cues (see below) or have a period very close or equal to 24 hours.
Spectral sensitivity of circadian photoreception
The neuroanatomical basis and photoreceptor mechanisms underlying the functional separation of visual and nonvisual responses to light have been discovered (for reviews see refs 76,77). Briefly, a novel opsin, melanopsin, has been located in specialized retinal ganglion cells that are directly sensitive to light and project to the brain areas mediating these nonvisual effects of light (eg, SCN for circadian and melatonin responses, olivary pretectal nuclei for pupil constriction responses). The cells are most sensitive to short-wavelength (blue) light ~ 480 nm and the absorption spectrum of melanopsin is distinct from the absorption spectra for the rods or cones. Animals that have had their melanopsin “knocked out” can still retain some circadian responses to light, showing that the traditional visual system likely contributes to these effects, but the melanopsin-driven system appears to be the primary phototransducer for the circadian effects of light. Action spectra for the behavioral effects of light in rodents and primates (eg, circadian phase resetting, pupil constriction) also show a peak sensitivity of - 480 nm, matching the cellular spectral sensitivity, as do action spectra for melatonin suppression and pupil responses in humans.Citation78-Citation80 Circadian phase resetting and the alerting effects of light are also short-wavelength sensitive in humans,Citation81-Citation86 suggesting that the novel non-rod, non-cone photoreceptor system primarily mediates a wide range of nonvisual effects of light. These findings are consistent with those in blind humans described above, who retain circadian responses to light despite absent or attenuated rod and cone function.
The effect of nonphotic time cues in the blind
Although light is the most powerful environmental time cue, nonphotic time cues are able to affect the circadian pacemaker.Citation30 In sighted subjects, the timing of sleep,Citation87 exercise,Citation88,Citation89 and carbohydrate intake,Citation90 but not knowledge of clock time,Citation91 have been shown to phase-shift the circadian clock. Other potential nonphotic synchronizers include social interaction and olfactory cues.Citation30 In the absence of light input to the clock, nonphotic time cues are obviously a potential therapeutic option to treat non-24-hour circadian rhythms disorder in the blind. There are currently no therapeutic guidelines, but some preliminary research suggests that it may be beneficial for patients to try to maintain a regular 24-hour schedule. Klerman and colleaguesCitation92 showed that the circadian system of a blind man with a period of 24.1 h became entrained when he lived on a 23.8 h “day.” AU aspects of his schedule were shifted simultaneously in this protocol including the sleep-wake cycle, meal times, activity, posture, and interaction with staff, precluding identification of the effective time signal, but collectively at least they were able to induce a phase advance. Other attempts to entrain circadian rhythms in blind people using a “potential complex ”zeitgeber“ including exercise (bicycle riding, 50 W over 15 mins), a strict social routine, a cold shower, and a heavy protein breakfastCitation37 appeared to have induced a shift in the timing of sleep and temperature rhythms, although it is not clear whether entrainment occurred. The relative weakness of nonphotic time cues is readily observed; however, in the majority of totally blind people who are not entrained when living in society (see above), where they are exposed to many 24-hour time cues such as work or school schedules, mealtimes, sleepwake schedules, activity, alarm clocks, family and social interaction, and so on. The inability to entrain to these schedules is dependent on an individual's intrinsic circadian period as the weak nonphotic time cues with have narrow ”limits of entrainment,“ the range of periods over which nonphotic cues can have an effect. If an individual's circadian period is too far from 24 hours, the weak nonphotic time signals will be unable to entrain it.
Treatment of circadian rhythm disorders in the blind
While some other drugs have been shown to shift the timing of the clock (for review, see ref 30) the most promising therapeutic strategy for treatment of non-24hour sleep-wake disorder is daily administration of melatonin. Although it was shown more than 20 years ago that melatonin treatment could entrain free running rhythms in ratsCitation93 and could cause phase advance shifts in humans,Citation94,Citation95 demonstration of entrainment in free running humans took longer to prove. Initial experiments using daily treatment with 5 mg or higher doses either failed to affect the circadian pacemaker at allCitation56,Citation96 or shortened period without inducing entrainment.Citation97,Citation98 These and other casesCitation99-Citation104 did report some improvement or stabilization of the sleep-wake cycle in these patients,Citation105 most likely through the direct soporific effects of melatonin.Citation105,Citation108
In 1996, we began a re-examination of the entraining effects of melatonin in seven men with non-24-hour rhythms with a period >24 hours.Citation109 Five subjects received 5 mg melatonin PO or placebo at 21:00 h each for a full circadian beat cycle (35 to 71 days depending on their circadian period) and two additional subjects received melatonin only in a single-blind design. Entrainment was assessed using urinary Cortisol rhythms.Citation64 As their endogenous rhythms were longer than 24 hours, subjects required a daily phase advance (ie, a shift to an earlier time) to become entrained to 24 hours.
Three of the subjects exhibited entrained Cortisol rhythms and one had a shortened period during treatment. The remaining three subjects were not affected by melatonin. Post-hoc analysis of melatonin treatment timing indicated that those subjects who failed to entrain had treatment initiated at a time that corresponded to the delay phase of the melatonin phase response curve (PRC)Citation110 (equivalent to -1:00-13:00 h in a normally-entrained subject) where melatonin causes a phase delay shift (ie, to a later time), the opposite of that required to entrain. Surprisingly, the subjects did not entrain once they free-ran into the correct window to cause a phase advance, unlike previous animal models.Citation93 Those subjects who became entrained or had a shortened period had their treatment initiated during the phase-advance portion of the PRC (-13:00-1:00 h in normal subjects), a time consistent with the observed daily advance achieved. We hypothesized at the time that the inappropriate initial timing in the nonentrained subjects may have affected the sensitivity to melatonin (for example, by receptor downregulation) when the appropriate treatment time was reached.
Shortly following publication of these data, similar results were published by Sack and colleagues using a 10-mg dose of melatonin initiated during the phase-advance window, who also showed entrainment of plasma melatonin rhythms when assessed during temporary suspensions of melatonin treatment.Citation111 In addition, they demonstrated that the 10-mg dose could be gradually stepped down to 0.5 mg and entrainment could be maintained.Citation111 These data raised the question as to whether a 0.5-mg de novo dose could also reset the clock, and both we and others confirmed that it could.Citation112-Citation114 This low dose was also more likely to entrain than treatment with higher doses (5 to 20 mg) maybe through providing a more discreet time signal than a higher dose with a more prolonged duration In the circulation. The Individual clrcadlan period may also affect the likelihood of entrainment with melatonin,Citation115 as those subjects with periods furthest from 24 hours may be outside the range of entrainment for this relatively weak time cue. Inconsistencies still exist, however, as to whether the circadian time of initial treatment affects subsequent entrainment. In our studies, using both 5 and 0.5 mg melatonin, entrainment was more likely if treatment was initiated in the advance, compared with the delay, phase of the PRC in both between and within-subjects designs (Citation109,Citation113, Lockley et al, unpublished results). At low doses, however, (0.5 mg or lower), melatonin treatment initiated at any circadian phase will eventually cause entrainment of the circadian pacemaker,Citation113-Citation114,Citation116 although there may be a delay until presumably the phase-advance part of the PRC is reached. Current consensus suggests, therefore, that smaller doses (up to 0.5 mg) may be preferable to larger doses, and that treatment timing should be timed initially to phase advance if possible (to achieve immediate entrainment (). Citation115 but if mistimed, may still eventually cause entrainment. Given melatonin's soporific properties, treatment should also be given close to the desired bedtime to ensure the alignment of the circadian and social day. Melatonin administration has also been explored for treatment of abnormal entrained phase disorders in the blind,Citation117 as well as sighted populations,Citation118 but appropriate timing may be even more important in these groups than non-24-hour sleep disorder.Citation119
Conclusion
The detrimental effects of loss of light perception, or loss of eyes, on circadian rhythm entrainment, and subsequently sleep and waking function, are often inadequately recognized by physicians, families, friends, and employers, making it difficult for blind people to obtain the treatment and support required to deal with this highly prevalent condition. Our data confirm the anecdotal accounts from subjects, who describe fighting to stay awake at work, having problems maintaining concentration and memory during the day, or being overwhelmed with a desire to sleep at inappropriate times. These circadian rhythm sleep disorders are chronic, unrelenting, and currently difficult to manage with conventional approaches. Simply treating the sleep-wake symptoms, for example with a combination of daytime stimulants and night-time hypnotics, indicates an insufficient diagnosis and a failure to address the underlying cause of the condition. Correcting the underlying misalignment between circadian and sleep-wake cycles, for example using appropriatelytimed melatonin treatment as described above, is fundamental for the optimal treatment of circadian rhythm sleep disorders.
Clinically, our data suggest that sleep disorders in visually impaired people with some degree of LP are not due to circadian desynchrony, and should therefore be investigated for other sleep disorders as in sighted subjects. Blind people with NPL who complain of sleep disorders, particularly episodic or cyclic insomnia and daytime sleepiness, should be studied longitudinally to confirm a circadian disorder diagnosis, using home-based sleep diary and urine assessments as described above.Citation61,Citation62 If non-24-hour rhythms are confirmed, then treatment with low-dose (0.5 mg) melatonin at a fixed clock time close to bedtime is warranted. To enhance the chance of immediate entrainment, treatment should commence once the subject begins to slip out of a normal sleep phase, characterized by difficulty initiating sleep (long sleep latency) or difficulty getting up in the morning. In advanced or delayed sleep phase syndrome, melatonin treatment timing should be individually determined based on the extent of their abnormal phase according the melatonin PRCCitation110 and stepwise treatment for particularly advanced or delayed subjects may be warranted. In all of these disorders, daily melatonin treatment is a lifelong requirement, as once treatment is stopped, the circadian pacemaker will revert to its endogenous period or phase angle (Figure 6), The safety profile of melatonin, while not assessed for very long-term use in humans, is good,Citation104,Citation120,Citation121 although care should be taken to ensure it is from a reliable source and pharmaceutical grade. In the near future, melatonin analogs will also become approved for this indication although as with melatonin, a correct initial diagnosis is required, and precise timing and dose remain to be determined.
Selected abbreviations and acronyms
| 11-OHCS | = | 11-hydroxycorticosteroid |
| aMT6s | = | 6-sulphatoxymelatonin |
| LP | = | light perception |
| NPL | = | no conscious perception of light |
| RHT | = | retinohypothalamic tract |
| SCN | = | suprachiasmatic nuclei |
The research reported herein was conducted at the University of Surrey and was supported by the South Thames Regional Health Authority, Institut de Recherches Internationale Servier, Stockgrand Ltd., University of Surrey and The Wellcome Trust (Grants 048197/Z/96/Z and 060018/B/99/Z). SWL is currently supported in part by the US Department of Defense (BC030928), the NIH National Center for Neurological Disorders and Stroke (R01NS040982), and the NIH National Center for Complementary and Alternative Medicine (R01AT002129). DJS is currently supported in part by grants from EU 6th Framework project EUCLOCK (No. 018741) and EU Marie Curie RTN grant (MCRTN-CT-2004-512362).
REFERENCES
- KneisleyLW.MoskowitzMA.LynchHJ.Cervical spinal cord lesions disrupt the rhythm in human melatonin excretion.J Neural Transm.1 97813(suppl)311323
- ZeitzerJM.AyasNT.SheaSA.BrownR.CzeislerCA.Absence of detectable melatonin and perservation of Cortisol and thyrotropin rhythms in tetraplegia.J Clin Endocrinol Metab.2000852189219610852451
- WehrTA.DuncanWC. Jr.SherL.et al.A circadian signal of change of season in patients with seasonal affective disorder.Arch Gen Psychiatry.2001581108111411735838
- ZeitzerJM.AyasNT.SheaSA.BrownR.Czeisler CA Absence of detectable melatonin and preservation of Cortisol and thyrotropin rhythms in tetraplegia.J Clin Endocrinol Metab.2000852189219610852451
- SaperCB.ScammellTE.LuJ.Hypothalamic regulation of sleep and circadian rhythms.Nature.20054371257126316251950
- BoulosZ.CampbellSS.LewyAJ.TermanM.DijkDJ.EastmanCI.Light treatment for sleep disorders: Consensus Report VII. Jet lag.J Biol Rhythms.1995101671767632990
- EastmanCI.BoulosZ.TermanM.CampbellSS.DijkDJ.LewyAJ.Light treatment for sleep disorders: Consensus Report. VI. Shift Work.J Biol Rhythms.1995101571647632989
- BarnesRG.DeaconSJ.ForbesMJ.ArendtJ.Adaptation of the 6-suIphatoxymelatonin rhythm in shiftworkers on offshore oil installations during a 2week 12-h night shift.Neurosci Lett.19982419129502203
- RajaratnamSM.ArendtJ.Health in a 24-h society.Lancet.20011358999100511583769
- FolkardS.TuckerP.Shift work, safety and productivity.Occup Med (Lond).2003539510112637593
- HamptonSM.MorganLM.LawrenceN.et al.Postprandial hormone and metabolic responses in simulated shift work.J Endocrinol.19961512592678958786
- RibeiroD.HamptonSM.MorganL.DeaconS.ArendtJ.Altered postprandial hormone and metabolic responses in a simulated shift work environment.J Endocrinol.19981583053109846159
- MorganL.ArendtJ.OwensD.et al.Effects of the endogenous clock and sleep time on melatonin, insulin, glucose and lipid metabolism.J Endocrinol.19981574434519691977
- KnutssonA.Health disorders of shiftworkers.Occup Med (Lond).20035310310812637594
- RogersHL.ReillySM.A survey of the health experiences of international business travelers. Part One - Physiological aspects.AAOHNJ.200250449459
- HastingsMH.ReddyAB.MaywoodES.A clockwork web: circadian timing in brain and periphery, in health and disease.Nat Rev Neurosci.2003464966112894240
- KleïtmanN.Sleep and Wakefulness. Chicago, III: University of Chicago Press.1 963
- HalbergF.SiffreM.EngelïM.HillmanD.ReinbergA.Etude en libre-cours des rythmes circadiens du pouls, de l'alternance veille-sommeil et de l'estimation du temps pendant les deux mois de séjour souterrain d'un homme adulte jeuneC R Acad Sci (Paris).19652601259126214275971
- WeverRA.The Circadian System of Man: Results of Experiments Under Temporal Isolation. New York, NY: Springer-Verlag.1979
- MiddletonB.StoneBM.ArendtJ.Human circadian phase in 12:12 h, 200: < 8 lux and 1000: < 8 lux light-dark cycles, without scheduled sleep or activity.Neurosci Lett.2002329414412161258
- WrightJr.KP, Hughes RJ, Kronauer RE, Dijk DJ, Czeisler CA. Intrinsic near24-h pacemaker period determines limits of circadian entrainment to a weak synchronizer in humans.Proc Natl Acad Sci U S A.200198140271403211717461
- WyattJK.Ritz-De CeccoA.CzeislerCA.DijkDJ.Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day.Am J Physiol.1999277R1152R116310516257
- CzeislerCA.DuffyJF.ShanahanTL.et al.Stability, precision, and near-24hour period of the human circadian pacemaker.Science.19992842177218110381883
- KellyTL.NeriDF.GrillJT.et al.Nonentrained circadian rhythms of melatonin in submariners scheduled to an 18-hour day.J Biol Rhythms.19991419019610452330
- MonkTH.BuysseDJ.BillyBD.KennedyKS.WillrichLM.Sleep and circadian rhythms in four orbiting astronauts.J Biol Rhythms.1998131882019615283
- DijkDJ.NeriDF.WyattJK.et al.Sleep, performance, circadian rhythms, and light-dark cycles during two space shuttle flights.Am J Physiol.2001281R1647R1664
- RossJK.ArendtJ.HomeJ.HastonW.Night-shift work in Antarctica: sleep characteristics and bright light treatment.Physiol Behav.199557116911747652039
- BroadwayJW.ArendtJW.Seasonal and bright light changes of the phase position of the human melatonin rhythm in Antarctica.Arctic Med Res.1988472012033272606
- LundJ.ArendtJ.HamptonSM.EnglishJ.MorganLM.Postprandial hormone and metabolic responses amongst shift workers in Antarctica.J Endocrinol.200117155756411739022
- MistlbergerRE.SkeneDJ.Nonphotic entrainment in humans?J Biol Rhythms.20052033935216077153
- RemlerO.Untersuchungen an Blinden ueber die 24-Stunden-Rhythmik.Monatsblaetter fuer Augenheilkunde.1 948113116137
- HoIIwichF.DieckhuesB.Circadian rhythm in the blind.J Interdiscipl Cycle Res.19712291302
- OrthDN.IslandDP.Light synchronization of the circadian rhythm in plasma Cortisol (17-OHCS) concentration in man.J Clin Endocrinol Metab.1969294794865779245
- KriegerDT.RizzoF.Circadian periodicity of plasma 11-hydroxycorticosteroid levels in subjects with partial and absent light perception.Neuroendocrinol.19718165179
- BodenheimerS.WinterJSD.FaïmanC.Diurnal rhythms of serum gonadotropins, testosterone, estradiol and Cortisol in blind men.J Clin Endocrinol Metab.1973374724754799034
- D'AlessandroB.BellastellaA.EspositoV.ColucciCF.MontalbettiN.Circadian rhythm of Cortisol secretion in elderly and blind subjects.BMJ.197422744827085
- MoogR.EndlichH.HildebrandtG.MartensH.Circadian rhythms in blind persons. In: Hildebrandt G, Moog R, Raschke F, eds.Chronobiology & Chronomedicine: Basic Research and Applications. Frankfurt am Main, Germany: Verlag Peter Lang;1987439441
- StavoskyJM.RosekindM.EnglandWR.MilesLEM.DementWC.Circadian rhythms of body temperature and sleep latency in blind subjects with sleep/wake complaints.Sleep Res.19909277
- LobbanMC.TredreB.Renal diurnal rhythms in blind subjects.J Physiol.19641702930
- SimenhoffML.Control of day-to-day salt excretion in man-Use of the blind subject as a model of its elucidation.Clin Res.196816396
- MigeonCJ.TylerFH.MahoneyJP.et al.The diurnal variation of plasma levels and urinary excretion of 17-hydroxycorticosteroids in normal subjects, night workers and blind subjects.J Clin Endocrinol Metab.19561662263313319454
- WeitzmanED.PerlowM.SassinJF.FukushimaD.BurackB.HellmanL.Persistence of the twenty-four hour pattern of episodic Cortisol secretion and growth hormone release in blind subjects.Trans Am Neurol Assoc.197397197199
- SchevingLE.KanabrockïEL.TsaiT.PaulyJE.Circadian and other variation in epinephrine and norepinephrine among several human populations, including healthy blinded and sighted subjects and patients with leprosy. In: Pauly JE, Scheving LE, eds.Advances in Chronobiology Part A. New York, NY: Alan R. Liss, Inc.1987329429
- SmithJA.O'HaraJ.SchiffAA.Altered diurnal serum melatonin rhythm in blind menLancet.19819336117710
- LewyAJ.NewsomeDA.Different types of melatonin circadian secretory rhythms in some blind subjects.J Clin Endocrinol Metab.198356110311076841552
- SackRL.LewyAJ.BloodML.KeithLD.NakagawaH.Circadian rhythm abnormalities in totally blind people: Incidence and clinical significance.J Clin Endocrinol Metab.1992751271341619000
- MilesLE.WilsonMA.High incidence of cyclic sleep/wake disorders in the blind.Sleep Res.19776192
- SasakiH.NakataH.MurakamiS.UesugïR.HaradaS.TeranishiM.Circadian sleep-waking rhythm disturbance in blind adolescence.Jpn J Psychiatry Neurol.1992462091635311
- LégerD.GuillemïnaultC.DefranceR.DomontA.PaillardM.Prevalence of sleep/wake disorders in persons with blindness.Clin Sci.19999719319910409474
- American Sleep Disorders Association.The International Classification of Sleep Disorders Diagnostic and Coding Manual. Rochester, Minn: American Sleep Disorders Association;1990362366
- MoseleyMJ.FouladiM.JonesHS.TobinMJ.Sleep disturbance and blindness, lancet.1996348151415158942795
- TabandehH.LockleySW.ButteryR.SkeneDJ.DefranceR.ArendtJ.Disturbance of sleep in blindness.Am J Ophthamol.1998126707712
- MilesLEM.RaynalDM.WilsonMA.Blind man living in normal society has circadian rhythms of 24.9 hours.Science.1977198421423910139
- OrthDN.BesserGM.KingPH.NicholsonWE.Free-running circadian plasma Cortisol rhythm in a blind human subject.Clin Endocrinol.197910603617
- OkawaM.NanamiT.WadaS.ShimizuT.HishikawaY.SasakiH.NagamineH.TakahashiK.Four congenitally blind children with circadian sleep-wake rhythm disorder.Sleep.1987101011103589322
- ArendtJ.AldhousM.WrightJ.Synchronisation of a disturbed sleep-wake cycle in a blind man by melatonin treatment,lancet.198817727732895305
- AldhousME.ArendtJ.Melatonin rhythms and the sleep-wake cycle in blind subjects.J Interdiscipl Cycle Res.1991228485
- NakagawaH.SackRL.LewyAJ.Sleep propensity free-runs with the temperature, melatonin and Cortisol rhythms in a totally blind person.Sleep.1992153303361519008
- KleinT.MartensH.DijkDJ.KronauerRE.SeelyEW.CzeislerCA.Chronic non-24-hour circadian rhythm sleep disorder in a blind man with a regular 24hour sleep-wake schedule.Sleep.1993163333438341894
- LockleyS.TabandehH.SkeneD.et al.Day-time naps and melatonin in blind people,lancet.1995; 1996346; 3471491 206
- LockleySW.SkeneDJ.ArendtJ.TabandehH.BirdAC.DefranceR.Relationship between melatonin rhythms and visual loss in the blind.J Clin Endocrinol Metab.199782376337709360538
- LockleySW.SkeneDJ.ButlerLJ.ArendtJ.Sleep and activity rhythms are related to circadian phase in the blind.Sleep.19992261662310450596
- SkeneDJ.LockleySW.ThapanK.ArendtJ.Effects of light on human circadian rhythms.Reprod Nutr Dev.19993929530410420432
- SkeneDJ.LockleySW.JamesK.ArendtJ.Correlation between urinary Cortisol and 6-sulphatoxymelatonin rhythms in field studies of blind subjects.Clin Endocrinol.1 99950715719
- ArendtJ.BojkowskiC.FraneyC.WrightJ.MarksV.Immunoassay of 6hydroxymelatonin sulfate in human plasma and urine: abolition of the urinary 24-hour rhythm with atenolol.J Clin Endocrinol Metab.198560116611723998065
- AldhousME.ArendtJ.Radioimmunoassay for 6-sulphatoxymelatonin in urine using an iodinated tracer.Ann Clin Biochem.1988252983033400987
- LockleySW.Human circadian rhythms: influence of light on circadian rhythmicity in humans. In: Squire LR, ed.New Encyclopaedia of Neuroscience, Oxford, UK: Elsevier. In press.
- MartensH.EndlichH.HildebrandtG.MoogR.Sleep/wake distribution in blind subjects with and without sleep complaints.Sleep Res.199019398
- CzeislerCA.WeitzmanED.Moore-EdeMC.ZimmermanJC.KnauerRS.Human sleep: Its duration and organization depend on its circadian phase.Science.1980210126412677434029
- LockleySW.SkeneDJ.TabandehH.BirdAC.DefranceR.ArendtJ.Relationship between napping and melatonin in the blind.J Biol Rhythms.19971216259104687
- LockleySW.DijkD-J.ArendtJ.SkeneDJ.Circadian and sleep-wake dependent control of alertness, mood and performance in field studies of blind subjects.Sleep.200124A4
- KerkhofGA.Van DongenHRA.Morning-type and evening-type individuals differ in the phase position of their endogenous circadian oscillator.Neurosci Lett.19962181531568945751
- RubergFL.SkeneDJ.HanifinJP.et al.Melatonin regulation in humans with color vision deficiencies.J Clin Endocrinol Metab.199681298029858768862
- CzeislerCA.ShanahanTL.KlermanEB.et al.Suppression of melatonin secretion in some blind patients by exposure to bright light.N Engl J Med.19953326117990870
- KlermanEB.ShanahanTL.BrotmanDJ.et al.Photic resetting of the human circadian pacemaker in the absence of conscious vision.J Biol Rhythms.20021754855512465888
- PeirsonS.FosterRG.Melanopsin: another way of signaling light.Neuron.20064933133916446137
- BrainardGC.HanifinJP.Photons, clocks, and consciousness.J Biol Rhythms.20052031432516077151
- BrainardGC.HanifinJP.GreesonJM.et al.Action spectrum for melatonin regulation in humans: Evidence for a novel circadian photoreceptor.J Neurosci.2001216405641211487664
- ThapanK.ArendtJ.SkeneDJ.An action spectrum for melatonin suppression: Evidence for a novel non-rod, non-cone photoreceptor system in humans.J Physiol.200153526126711507175
- HankinsMW.LucasRJ.The primary visual pathway in humans is regulated according to long-term light exposure through the action of a nonclassical photopigment.CurrBiol.200212191198
- WarmanVL.DijkDJ.WarmanGR.ArendtJ.SkeneDJ.Phase advancing human circadian rhythms with short wavelength light.Neurosci Lett.2003342374012727312
- LockleySW.BrainardGC.CzeislerCA.High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength lightJ Clin Endocrinol Metab.2003884502450512970330
- CajochenC.MunchM.KobialkaS.et al.High sensitivity of human melatonin, alertness, thermoregulation, and heart rate to short wavelength light.J Clin Endocrinol Metab.2005901311131615585546
- RevelIVL.ArendtJ.TermanM.SkeneDJ.Short-wavelength sensitivity of the human circadian system to phase-advancing light.J Biol Rhythms.20052027027215851533
- LockleySW.EvansEE.ScheerFAJL.BrainardGC.CzeislerCA.AeschbachD.Short-wavelength sensitivity for the direct effects of light on alertness, vigilance, and the waking electroencephalogram in humans.Sleep.20062916116816494083
- RevelIVU.ArendtJ.FoggLF.SkeneDJ.Alerting effects of light are sensitive to very short wavelengths.Neurosci Lett.20063999610016490309
- DanilenkoKV.CajochenC.Wirz-JusticeA.Is sleep per se a zeitgeber in humans.J Biol Rhythms.20031817017812693871
- BuxtonOM.LeeCW.L'Hermïte-BalérïauxM.TurekFW.Van CauterE.Exercise elicits phase shifts and acute alterations of melatonin that vary with circadian phase.Am J Physiol.2003284 R714R724
- BargerLK.WrightJr. KP.HughesRJ.CzeislerCA.Daily exercise facilitates phase delays of circadian melatonin rhythm in very dim light.Am J Physiol.2004286R1077R1084
- KràuchiK.CajochenC.WerthE.Wirz-JusticeA.Alteration of internal circadian phase relationships after morning versus evening carbohydrate-rich meals in humans.J Biol Rhythms.20021736437612164252
- MiddletonB.ArendtJ.StoneBM.Human circadian rhythms in constant dim light (8 lux) with knowledge of clock time.J Sleep Res.1996569768795806
- KlermanEB.RimmerDW.DijkDJ.KronauerRE.RizzoJF.IIICzeislerCA.Nonphotic entrainment of the human circadian pacemaker.Am J Physiol.1998274R991R9969575961
- RedmanJ.ArmstrongS.NgKT.Free-running activity rhythms in the rat: entrainment by melatonin.Science.1983219108910916823571
- ArendtJ.BorbélyAA.FraneyC.WrightJ.The effects of chronic, small doses of melatonin given in the late afternoon on fatigue in man: A preliminary study.Neurosci Lett.1984453173216728321
- ArendtJ.BojkowskiC.FolkardSF.et al.Some effects of melatonin and the control of its secretion in humans. In: Evered D, Clark S, eds.Photoperiodism, Melatonin and the Pineal. London, UK: Pitman.1985266283
- FolkardS.ArendtJ.AldhousM.KennettH.Melatonin stabilises sleep onset time in a blind man without entrainment of Cortisol or temperature rhythms.Neurosci Lett.19901131931982377316
- SackRL.LewyAJ.HobanTM.Free-running melatonin rhythms in blind people: phase shifts with melatonin and triazolam administration. In: Rensing L, an der Heiden U, Mackey MC, eds.Temporal Disorder in Human Oscillatory Systems. Heidelberg, Germany: Springer-Verlag;1987219224
- SackRL.LewyAJ.BloodML.StevensonJ.KeithLD.Melatonin administration to blind people: Phase advances and entrainment.J Biol Rhythms.199162492611773095
- SarrafzadehA.Wirz-JusticeA.ArendtJ.EnglishJ.Melatonin stabilises sleep onset in a blind man. In: Home J, ed.Sleep '90. Bochum, Germany: Pontenagel Press19905154
- PalmL.BlennowG.WetterbergL.Correction of non-24-hour sleep/wake cycle by melatonin in a blind retarded boy.Ann Neurol.1991293363392042950
- TzischinskyO.PalI.EpsteinR.DaganY.LavieP.The importance of timing in melatonin administration in a blind man.J Pineal Res.1992121051081507054
- JanJE.EspezelH.AppletonRE.The treatment of sleep disorders with melatonin.Dev Med Child Neurol.199436971078132132
- LapierreO.DumontM.Melatonin treatment of a non-24-hour sleep-wake cycle in a blind retarded child.Biol Psychiatry.19951191227578644
- ArendtJ.SkeneDJ.MiddletonB.LockleySW.DeaconS.Efficacy of melatonin treatment in jet lag, shift work, and blindness.J Biol Rhythms.1997126046179406036
- CramerH.RudolphJ.ConsbruchU.KendelK.On the effects of melatonin on sleep and behavior inman. Adv Biochem Psychopharmacol.197411187191
- LavieP.LuboshitzkyR.Melatonin: Possible role in human sleep and reproduction. In: Hayaishi O, Inoue S, eds.Sleep and Sleep Disorders: Molecule to Behavior. Tokyo, Japan: Academic Press;1997209222
- ZhdanovaIV.WurtmanRJ.Efficacy of melatonin as a sleep-promoting agentJ Biol Rhythms.1997126446509406040
- CajochenC.KràuchiK.Wirz-JusticeA.The acute soporific action of daytime melatonin administration: effects on the EEG during wakefulness and subjective alertness.J Biol Rhythms.1997126366439406039
- LockleySW.SkeneDJ.JamesK.ThapanK.WrightJ.ArendtJ.Melatonin administration can entrain the free-running circadian system of blind subjects.J Endocrinol.2000164R1R610607943
- LewyAJ.AhmedS.JacksonJML.SackRL.Melatonin shifts human circadian rhythms according to a phase-response curve.Chronobiol Int.199293803921394610
- SackRL.BrandesRW.KendallAR.LewyAJ.Entrainment of free-running circadian rhythms by melatonin in blind people.N Engl J Med.20003431070107711027741
- LewyAJ.BauerVK.HaslerBP.KendallAR.PiresLN.SackRL.Capturing the circadian rhythms of free-running blind people with 0.5 mg melatonin.Brain Res.20019189610011684046
- HackLM.LockleySW.ArendtJ.SkeneDJ.The effects of low-dose 0.5-mg melatonin on the free-running circadian rhythms of blind subjects.J Biol Rhythms.20031842042914582858
- LewyAJ.EmensJS.LeflerBJ.YuhasK.JackmanAR.Melatonin entrains free-running blind people according to a physiological dose-response curve.Chronobiol Int.2005221093110616393710
- LewyAJ.HaslerBP.EmensJS.SackRL.Pretreatment circadian period in free-running blind people may predict the phase angle of entrainment to melatonin.Neurosci Lett.200131315816011682151
- LewyAJ.EmensJS.BernertRA.LeflerBJ.Eventual entrainment of the human circadian pacemaker by melatonin is independent of the circadian phase of treatment initiation: clinical implications.J Biol Rhythms.200419687514964705
- SkeneDJ.ArendtJ.Circadian rhythm sleep disorders in the blind and their treatment with melatonin.Sleep Med.2007865165517420154
- ArendtJ.SkeneDJ.Melatonin as a chronobiotic.Sleep Med Rev.20059253915649736
- LockleySW.Timed melatonin treatment for delayed sleep phase syndrome: the importance of knowing circadian phase.Sleep.2005281214121616295202
- ArendtJ.Safety of melatonin in long-term use(?).J Biol Rhythms.1997126736819406044
- HerxheimerA.Does melatonin help people sleep.BMJ.2006332 37337416484240