Background
The number of injured far exceeds those dead and the average injury to mortality ratio in earthquakes stands at 3:1. Immediate effective medical response significantly influences injury outcomes and thus the overall health impact of earthquakes. Inadequate or mismanagement of injuries may lead to disabilities. The lack of precise data from immediate aftermath is seen as a remarkable weak point in disaster epidemiology and warrants evidence generation.
Objective
To analyze the epidemiology of injuries and the treatment imparted at a secondary rural hospital in the Kutch district, Gujarat, India following the January 26, 2001 earthquake.
Design/Methods
Discharge reports of patients admitted to the hospital over 10 weeks were analyzed retrospectively for earthquake-related injuries.
Results
Orthopedic injuries, (particularly fractures of the lower limbs) were predominant and serious injuries like head, chest, abdominal, and crush syndrome were minimal. Wound infections were reported in almost 20% of the admitted cases. Surgical procedures were more common than conservative treatment. The most frequently performed surgical procedures were open reduction with internal fixation and cleaning and debridement of contaminated wounds. Four secondary deaths and 102 transfers to tertiary care due to complications were reported.
Conclusion
The injury epidemiology reported in this study is in general agreement with most other studies reporting injury epidemiology except higher incidence of distal orthopedic injuries particularly to the lower extremities. We also found that young males were more prone to sustaining injuries. These results warrant further research. Inconsistent data reporting procedures against the backdrop of inherent disaster data incompleteness calls for urgent standardization of reporting earthquake injuries for evidence-based response policy planning.
Introduction
Over 281 earthquakes occurred in 58 countries between 1996 and 2005, causing more than 162,986 deaths, and affecting over 39 million people Citation1. The number of injured far exceeds those dead Citation2; and the average injury to mortality ratio in earthquakes stands at around 3:1 for the above mentioned time period (SD = 12.5; own calculation based on data from www.em-dat.be). Immediate effective medical response significantly influences injury outcome and thus the overall health impact of earthquakes. Inadequate or mismanagement of injuries may lead to infections and disabilities and contribute to creating future vulnerabilities. This is of particular relevance in developing countries, especially in Asia where most earthquakes strike densely populated areas Citation3.
Lack of precise data from immediate aftermath is seen as a remarkable weak point in disaster epidemiology Citation3–Citation5. This is particularly the case, since compiling injury data in the early stages of an earthquake is rather unwelcome as the main focus, and rightly so, is upon saving lives and surging capacity for adequate response.
Earthquakes have a narrow warning period. Therefore, the points of entry for mitigating their health impacts include primarily anti-seismic building, early rescue, and effective first aid Citation3 Citation4 Citation6. The prohibitive costs of seismic hazard proof construction compromises the adherence to and the implementation of anti-seismic building codes in most developing countries. The information on injury patterns from previous earthquakes then becomes crucial in guiding effective preparedness and successful response programs in resource poor settings.
The last earthquake with its epicenter in India was the Gujarat earthquake of January 26, 2001. The epicenter was located in the North-East of Bhuj city and the quake affected over 8,792 villages in 171 Talukas (governmental administrative units) of the 21 districts in Gujarat Citation7 Citation8. Human impact of the earthquake involved 20,005 deaths and over 166,812 (including 20,717 ‘serious’) injuries Citation7. The district of Kutch accounted for more than 92% of the deaths and 82% of the total injuries reported Citation8.
Primary failure of the health care facilities in the district due to structural damage delayed much required early response. The G.K General civil hospital, a crucial secondary health facility in the area, was completely damaged Citation7 Citation8. Almost all of the hospital facilities in Kutch were destroyed including 2 hospitals, 8 community health centers, 42 primary health care centers, 37 dispensaries, and 227 sub-centers Citation7 Citation8. Sarvodaya hospital, a trust-based hospital in Bidada village, was one of the few intact health care facilities. As a result there was heavy influx of patients from other areas of the district to the centre, even when it is located over 60 kilometers from the epicenter.
The rationale of this paper is to further the knowledge of the injury epidemiology after earthquakes by examining injury patterns, treatments, and patient outcomes based on secondary data from the Bidada Sarvodaya hospital. The study aims to highlight the challenges of injury data reporting and recording in terms of quantity and quality.
Methods
Design
The study is a retrospective analysis of secondary data obtained from the discharge reports of patients treated at the Bidada Sarvodaya Hospital, Kutch, Gujarat, India following the earthquake of January 26, 2001.
Procedures
The study was completed in August 2007. Approval for the site visit was obtained from the Director of the Bidada Rehabilitation Centre. Access to these data resulted from the author's own work in the Bidada hospital during the earthquake in 2001 within a relief and rehabilitation project.
Sample
Patients treated for earthquake-related injuries and illnesses in the hospital over the 10-week post-quake period (January 26, 2001–April 4, 2001) were included in the study. The inclusion criteria were as follows: injuries that were recorded as having resulted from the January 26, 2001 earthquake in the discharge reports for which in-patient health care was sought and that had not resulted in death.
Analyses
The discharge reports of 1,248 patients treated at the hospital during the 10-week period were reviewed manually for sex, age, village for geographic origin, date of admission, date of discharge, diagnosis, injury types (compound/crush/multiple/softtissue), anatomical side of injury, type of fractures, presence of infection, treatment imparted, hospital procedure performed, and outcome of treatment (including transfer to tertiary care).
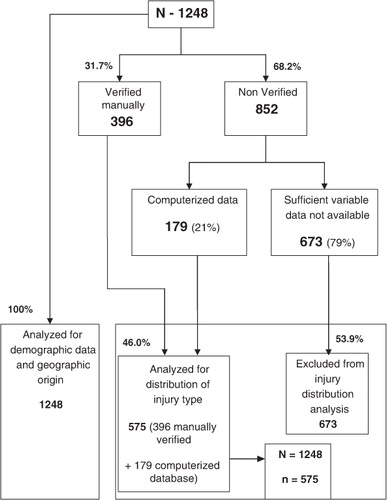
Although demographic data was available for a majority of the 1,248 patients, analyzable data on other identified variables was available only on 396 (31.7%) patients in the paper-based discharge reports. Since the admissions-related data of these 1,248 patients was also maintained partially in an electronic database, a careful cross-matching by serial number, name, age, sex, and geographic origin of the patients was done both in the paper-based forms and the electronic data base and data of 179 additional patients was obtained from the electronic database. Thus a total of 575 of the 1,248 (46%) patient reports (including 396 paper-based reports and 179 electronic reports) were analyzable for distribution of injury (or other condition) by frequency and were included in the study. Depending on the availability of information on a particular variable in the discharge reports, the total number of cases studied for that variable (n) changes and is specified in the results section.
The data obtained was entered in Microsoft Excel: Mac for descriptive analysis. All of the 1,248 discharge reports were included in the analysis of geographical origin and the demographic data of age and sex (see ).
Figure 1. Structure of the database.
Results
Demographic information
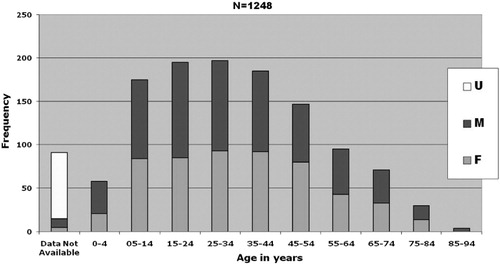
Of the 1,248 case reports 100 (8.0%) had missing information for the village of origin. Over half of the patients (51%) came from the epicenter city of Bhuj, probably since the civil hospital (G.K General Hospital) in Bhuj had collapsed. There were 1,157 (91, 7.2% missing) and 1,172 (76, 6.0% missing) cases that were analyzed for age and gender distribution, respectively. The mean age of the patients treated at the hospital was 30.7 years (SD = 20.87) with a range of 0 to 90 years. A total of 314 (27.1%) individuals were 18 years old or younger and 136 (11.8%) were 60 years or older. The data showed a predominance of middle-aged males (see ). The gender distribution of the study group was quite uniform with 621 (53.0%) males and 551 (47.0%) females.
Figure 2. Age and gender distribution of the sample.
Admissions and discharges
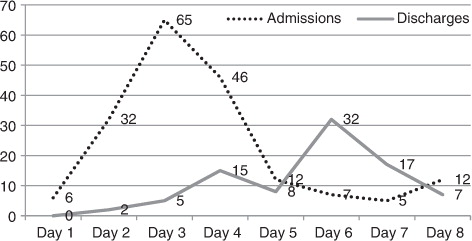
A total of 185 admissions (highest for a week) and 86 discharges were recorded in the first week with maximum admissions on day 2 (see ) and uniform distribution from week 2 to 10. The number of discharged per day peaked on day 5 with the admissions returning to baseline on day 6. There was a second wave of admissions (15 admissions) that peaked on day 9 after the earthquake. The number of discharges increased in the last week (March 26 – March 31, 2001). No new admissions were recorded during this period.
Figure 3. Admissions (n = 185) and discharges (n=86) in the first 8 days after the earthquake.
Length of stay
A total of 420 patients were analyzed for the duration of the hospital stay, which ranged from 0 to 64 days. Of the 35.3% of patients that were hospitalized for less than a week, a majority of them (25.3%) stayed between 2 to 4 days. The highest number of patients 45 (10.7%) stayed for a period of 3 days followed by 40 (9.5%) who stayed for 2 days.
Clinical analysis of the injuries
Type of injury
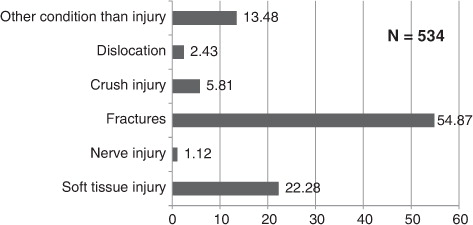
There were 534 cases that could be analyzed for type of injury. With 293 cases, fractures (51%) were recorded as the most predominant type of injury followed by soft tissue injuries (119, 20.7%) that mainly included cuts, bruises, contusions, and lacerations. Thirty-one cases (5.4%) of crush injury were reported. Dislocations (13, 2.3% of all analyzed cases) were less frequent. Six nerve injuries included brachial plexus Citation3, radial nerve Citation2, and radio-ulnar nerve Citation1. A total of 72 (12.1%) cases had other health conditions than injuries while these were still claimed to be related to the earthquake in the discharge reports (see ). Forty-one cases were not specified and could be amputations, contusions, concussions (12 head injuries), internal injuries/organ damage, or multiple types.
Figure 4. Types of injuries.
Anatomical location of injury
There were 463 cases that could be analyzed for anatomical location of the injury. A total of 136 patients were reported having multiple injuries (29.4%) with compound injuries in 76 cases (16.2%). A total of 441 reports identified the side of injury. The injuries sustained to the left (173, 39.2%) were marginally higher than the right side (154, 34.9%). The incidence of axial and bilateral injuries was 67 (15.2%) and 47 (10.7%), respectively.
Extremity injuries (266, 57.4%) predominated followed by injuries of the pelvis (24, 5.2%). Two cases of abdominal injury were of burst abdomen type. Head injury (12, 2.6%) included mainly fractures of the mandible. Chest injuries (11, 2.4%) included multiple fractures of the ribs, of which three cases required inter-costal drain tube insertion for restoring respiratory function. Spinal injuries were quite low (12, 2.6%) and two cases of paraplegia were reported.
Types of fractures and dislocations
Of the fractures (see ), extremity fractures were by far the most reported (87.4%). Upper extremity fractures were less frequent at 52 (20.3%) than lower extremity fractures 204 (79.7%). Nine patients (3.0%) reported fractures of both upper as well as lower extremities. Lower extremity, particularly tibia-fibular (38.6%) and femur (22.2%) fractures were the most common type of lower extremity fractures, whereas radius-ulna fractures were predominant in upper extremity fractures (9.6%).
Figure 5. Anatomical location of fractures.
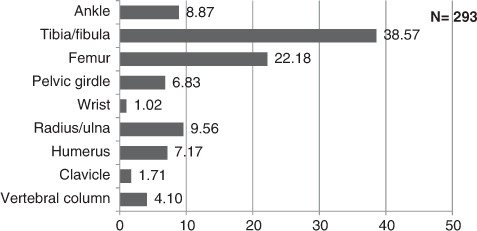
Ankle fractures (8.9%) were more common compared to wrist (1.0%) fractures. Pelvic girdle fractures (6.8%) mainly included acetabular and pubic-rami fractures. Vertebral fractures (4.1%) were of burst nature. Crush injuries were mainly of the hand and foot. Dislocations included ankle dislocations (4, 31%) followed by hip (3, 23%), radius-ulna (2, 15%), and shoulder joint (2, 15%). Wrist and elbow dislocations were reported 1 of each, (8%).
Wound infections
A total of 78 of the 503 patients with injuries (15.5%) reported infected wounds at the time of admission. The cases were uniformly distributed over the 10-week period despite the total increase in the number of admissions in week 4, 7, and 8, respectively.
Other health conditions
Of the 72 cases that had health conditions other than injuries; the single most common complaint was hernia (10 cases) followed by 9 (12.5%) cases of COPD, 6 (8.3%) cases of diabetic complications, 4 (5.5%) cases of tuberculosis, and 4 (5.5%) of ischemic heart disease (see ). These cases are excluded from the anatomical analysis but included in analysis of treatment. These are probably the 71 cases that only received medications.
Table 1. Non-injury conditions treated at the hospital during 10-week period
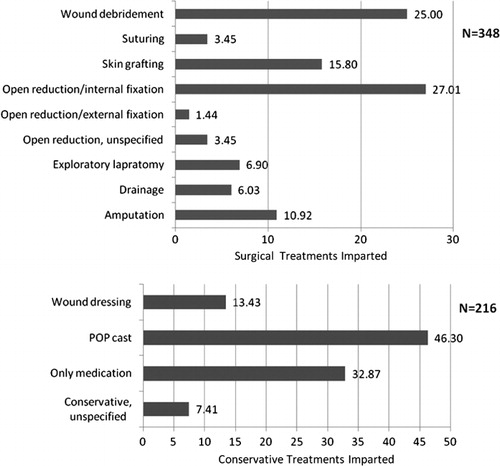
Treatment
There were 564 cases that could be analyzed for treatment. Operative (61.7%) was more common than conservative treatment. Plaster of paris (POP) cast for closed fractures was the most often used conservative procedure followed by the prescription of medications and wound dressing (see ). Open reduction and internal fixation was the most common surgical procedure followed by wound debridement and skin grafting. This corresponds to the finding that fractures and soft tissue injuries were the two major types of injuries sustained.
Figure 6. Anatomical location of fractures.
A total of 38 amputations (6.7%) were recorded. Of these, below-ankle amputations involving the foot (36%) were most frequent followed by below-knee amputations (26%). This is in accordance with the findings regarding crush injuries that were more common in the foot and the most common fractures in distal tibia-fibular bones.
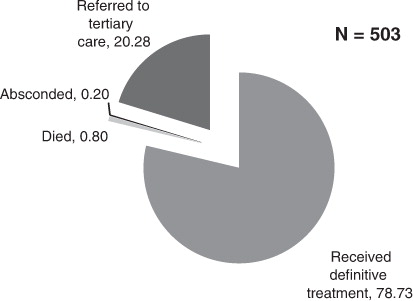
Patient outcomes
The definitive outcomes are as shown in . Four deaths occurred during the study period. The cause of death in these patients was not ascertained as the case reports were sent to the coroners. A total of 102 patients were transferred to tertiary care for further management.
Figure 7. Patient outcomes with regard to treatments imparted.
Discussion
Although our findings were in general agreement with other studies reporting injury epidemiology after earthquakes, we report higher incidence of orthopedic injuries, particularly extremity fractures of the lower limbs (tibia-fibula, femur, radius-ulna, and humerus in this order of frequency), in our study. Although the location of person when injury occurs and the behavior has been documented as possible reasons for the nature of injury sustained Citation9, there is lack of substantial evidence to make these correlations with currently available data. Head, spine, and chest injuries were comparatively low, which may be attributed to poor rescue and response operations in Gujarat Citation4.
The study reports a higher proportion of young males (25–45 years) as compared to other studies from Gujarat Citation7 Citation8 which is challenging to explain. Two of the four studies from Gujarat reported more female patients than males, one study did not mention this information and one found no gender difference Citation7 Citation8 Citation10. One of the reasons could be that there is a marginal predominance of middle aged males in the population of the Kutch district Citation11. However, since the exact proportion in the affected population is unavailable, it is less pragmatic to make the association. Similar inconsistencies are reported in other studies that report gender as a vulnerability factor for injuries although it was not statistically correlated. A further investigation about the social structure and gender equation of the society and its influence in health seeking behavior alongside a thorough statistical analysis of injury data may provide useful information in resolving these anomalies.
The average duration of hospital stay in the patients was 2–4 days with a wide range of 0–64 days. Bidada is a not-for-profit charitable hospital and provided free food and lodging for the patients and their relatives after the earthquake, which may be the reason for extended stay of several patients. Duration of hospital stay after the disaster is an important variable particularly to inform humanitarian response strategies. However, limited data exists on these and further research in this direction should be initiated.
Secondary deaths (deaths after rescue) are relatively low following earthquakes and have been associated with the efficiency of the search and rescue performance Citation12. If a greater number of serious injuries are rescued alive, then although primary mortality (impact deaths) is low, the secondary mortality may rise proportionately Citation13. This was also the case with the Gujarat earthquake where rescue efforts were severely criticized. Our study reports four secondary deaths. The actual cause of death for these patients remained unknown due to missing and incomplete documentation. The number of secondary deaths may have been largely underestimated. Also, low mortality in this study may be related to the fact that only a small number of serious injuries were treated and that more serious cases were transferred to tertiary care.
Soft tissue injuries were reported in 119 of the cases. Fifteen percent of the fractures sustained were with open wounds. Proportionately, around 26% of the operation theatre procedures were cleaning and debridement of contaminated wounds (see ). Moderate and serious injuries requiring admission were better reported than minor soft tissue injuries that are often treated at site or on an outpatient basis by simple first aid techniques to prevent unnecessary overcrowding of hospitals and to allow effective use of scarce resources. This leads to an unintentional selective exclusion of minor injuries from the reports. This is critical given that most earthquake injuries are soft tissue injuries resulting from falling objects or debris. Two reasons for a high number of minor soft tissue injuries being treated on an indoor basis at the hospital were first the individual delay in seeking health care that led to complications, and second the long commuting distances that made travel for most patients both logistically and monetarily less feasible for daily dressings. People with lost homes preferred to stay in the hospital tents where food and accommodation was provided free of cost for accompanying family members as well.
Soft tissue injuries are more prone to primary and secondary infections. Most injuries after earthquakes are either contaminated and/or infected. This has been confirmed by our study with wound infection present in over 65% of the soft tissue injuries. Although the risk of tetanus is a major concern following disasters, few studies address it Citation14. Limited information is available about the hospital-acquired secondary infections despite that adequate hygiene in mass casualty situations is problematic Citation15. In Gujarat, generally low rates of secondary post-operative infections were reported. Partly due to the high sensitivity of the rural population to antibiotics that were largely unused in these areas Citation8. This finding was similar in this study. Over the 10 weeks, the secondary infection rates remained low probably also indicating appropriate post-operative care.
The number of non-fatal serious injuries including amputations, chest, abdominal burst, head, and spinal cord injuries were limited to around 13% in this study. Thirty-one cases of crush injuries are reported. Most of them were managed conservatively. However, cases with gangrene (death of tissue due to inadequate blood supply and superadded infections) required elective amputation (surgical removal or loss of a body part). Crush injuries of the foot were more common and, correspondingly, 14 below ankle amputation (36%) were reported.
Children are more prone to crush syndrome following crush injuries and also develop acute renal failure at a higher rate. Since they are more difficult to diagnose both clinically and diagnostically, close monitoring of children is solicited to detect early signs Citation16. The age distribution for crush injuries was uniform in the study with no significant increase in the pediatric or geriatric age group. No cases of crush syndrome were recorded in this study.
Amputations and traumatic paraplegia (paralysis of both lower limbs usually a result of spinal fractures involving damage to the spinal cord) are the most common permanent disabilities resulting from earthquake injuries. There were two cases of spinal cord injury that later developed paraplegia. Peripheral nerve injuries (PNI) leading to distal paralysis also accounts for permanent disability. Nerve injuries reported in the study include brachial plexus injury Citation3, radial nerve Citation2, and radio-ulnar nerve Citation1, respectively. Thus, at least 11% of cases with permanent bodily impairments were found in this study.
In post-disaster conditions, physical disabilities may also result from unintentional negligence, inadequate, or mismanaged injuries due to lack of infrastructure availability at a mass scale. A study conducted 2 years after the Gujarat earthquake reported 10% of the injuries (mainly spinal in multiple injury and double fractures) were missed during diagnosis and over 30.5% patients underwent re-surgeries, 23% had non-union, and 12% experienced joint range of motion (ROM) restriction. Re-assessment and review of all patients before discharge is necessary to detect missed injuries and, more importantly, standardized procedures Citation17 and training in mass casualty management for surgeons and medical staff should be mandatory Citation18.
Aggressive orthopedics, especially with respect to implant operations, was observed along with serious compromises in implant type after the Gujarat earthquake Citation8. In total, 76 of the 575 cases in the study (13%) were open compound fractures. External fixation is mandated in open contaminated fractures. However, the number of external fixations were a mere 5 (1%) cases. Conversely, internal fixations were comparatively high at 94 (17%). Bidada hospital also faced lack of continuous competent human resources. Post-operative management was occasionally compromised due to the short-term commitments offered by the volunteers. The surgeons often operated and left within a week or visited in rotations. Often the coordination amongst the therapeutic plans of one surgeon and the next one was difficult (17,19,20).
In parts of Gujarat, external devices that were new to local specialists were used. These were initially effective but led to complications due to delay in removal resulting in high number of re-surgeries Citation10. The competence of local orthopedic surgeons is critical when deciding complex therapies that achieve near similar results to standard local practices. However, it may be incorrect to judge the surgical decisions in disaster situations, retrospectively. Especially in view of the availability of fixation instruments at a specific time and the need for clinical accuracy. These factors may explain the surgical cases at Bidada hospital long after the initial phase was over. It is therefore necessary that appropriate minimum standards for surgical care in emergencies are formulated and existing guidelines are implemented extensively to prevent iatrogenic disabilities (Citation17, Citation19, Citation21).
Physical disability is an enormous psychological and financial burden on the population in terms of resources. Activities of daily living and, more importantly, income generation are greatly affected contributing to future vulnerabilities. A study in Japan showed that individuals with physical disabilities were 5.6 times more vulnerable to earthquake impacts Citation22. However, disabilities – both partial and permanent – are often neglected after earthquakes (this relates to the personal observation of the author during her work in Gujarat after the earthquake). Since orthopedic trauma constitutes the bulk of the injuries after earthquakes, non-union and mal-union of fractures should be monitored closely for the risk of mis-management (Citation2,Citation23,Citation24).
Additionally, data completeness was a major issue in our study similar to other studies Citation6–Citation8 Citation12 Citation13 Citation18 Citation24–Citation27 reporting injury epidemiology. Less than half (575, 46%) reports were analyzable. There is currently no agreement on standardized methodology to assess and/or report disaster injuries. Although a large number of scattered international disaster databases exist, most only report consolidated numbers of those injured. In the wake of the increase in the frequency of earthquakes and their human impacts in the recent past, urgent coordinated standardization is a pressing need to help collect robust evidence to guide preparedness and emergency response programmers globally. The Sphere project Citation28 is one step in this direction and data to feed information to such efforts is the need of the hour.
The authors propose developing a simple patient case reporting form for injury data reporting in the early phases of earthquakes as a first step to standardization. Information on the types, nature, and mechanism of injuries sustained should be collected on the basic form preferably printed behind triage tags. Additionally, the use of low-cost, electronic handheld devices like a PDA with Optical Character Recognition software (OCR) should be considered to speed up data entry directly from paper-based forms to electronic databases. Completeness may still be an issue but this approach will help reduce the time required to record, transfer, and process data in emergencies hence contributing meaningful information to inform response policies Citation20.
In conclusion, our study could confirm basic data from other hospital-based discharge report studies including those from Gujarat Citation22 Citation23. However, few inconsistent findings related to the age, gender distribution, and nature of injuries mandate further investigations. It is likely that this study underestimated the number of serious injuries and permanent impairments due to incomplete documentation and transfers to tertiary institutions. Future research examining cases that are not well documented and collecting data on functional health Citation2 is warranted to close this knowledge gap.
Conflict of interest and funding
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Related Research Data
References
- Centre for Research on the Epidemiology of Disasters. Newsletter issue no. 5 2006. Available from: http://www.cred.be/publication/credcrunch-2.
- Reinhardt JD, Li J, Gosney J, Rathore F, Haig AJ, Mark M, DeLisa J, et al. Disability and medical rehabilitation in international disaster relief. GHA. 2011; (in press) Accepted June 23 2011.
- Guha-Sapir D, Vos F. Chapter 2: earthquakes, an epidemiological perspective on patterns and trends. Human casualties in earthquakes: progress in modelling and mitigation. Spence R, So E, Scawthorn CSpringer. New York, 2011; 13–24.
- Lechat MF. Disasters and public health. Bull World Health Organ. 1979; 57: 11–17.
- Lechat MF. The epidemiology of health effects of disasters. Epidemiol Rev. 1990; 12: 192–8.
- Peek-Asa C, Ramirez M, Seligson H, Shoaf K. Seismic, structural, and individual factors associated with earthquake related injury. Inj Prev. 2003; 9: 62–66. 10.3402/gha.v4i0.7196.
- Roy N, Shah H, Patel V, Coughlin RR. The Gujarat earthquake 2001 experience in a seismically unprepared area: community hospital medical response. Prehosp Disaster Med. 2002; 17: 186–95.
- Roy N, Shah H, Patel V, Bagalkote H. Surgical and psychosocial outcomes in the rural injured – a follow-up study of the 2001 earthquake victims. Injury. 2005; 36: 927–34. 10.3402/gha.v4i0.7196.
- Dhar S, Halwai M, Ramzan M, Wani M, Butt M, Bhat M, et al.. The Kashmir earthquake experience. Eur J Trauma. 2007; 33: 74–80. 10.3402/gha.v4i0.7196.
- Jain V, Noponen R, Smith BM. Pediatric surgical emergencies in the setting of a natural disaster: experiences from the 2001 earthquake in Gujarat, India. J Pediatr Surg. 2003; 38: 663–7. 10.3402/gha.v4i0.7196.
- Government of Gujarat: health statistics Gujarat 2009–10. In: Statement – 14, District wise distribution of population (in percentage) by age and sex, 2001. Division VS, ed. Gandhinagar, Gujarat State: Commissionerate of Health, Medical Services, Medical Education and Research; 2011 p. 54.
- de Bruycker M, Greco D, Annino I, Stazi MA, de Ruggiero N, Triassi M, et al.. The 1980 earthquake in southern Italy: rescue of trapped victims and mortality. Bull World Health Organ. 1983; 61: 1021–5.
- Tanaka H, Oda J, Iwai A, Kuwagata Y, Matsuoka T, Takaoka M, et al.. Morbidity and mortality of hospitalized patients after the 1995 Hanshin-Awaji earthquake. Am J Emerg Med. 1999; 17: 186–91. 10.3402/gha.v4i0.7196.
- Waring SC, Brown BJ. The threat of communicable diseases following natural disasters: a public health response. Disaster Manag Response. 2005; 3: 41–47. 10.3402/gha.v4i0.7196.
- Oncul O, Keskin O, Acar HV, Kucukardali Y, Evrenkaya R, Atasoyu EM, et al.. Hospital-acquired infections following the 1999 Marmara earthquake. J Hosp Infect. 2002; 51: 47–51. 10.3402/gha.v4i0.7196.
- Iskit SH, Alpay H, Tugtepe H, Ozdemir C, Ayyildiz SH, Ozel K, et al.. Analysis of 33 pediatric trauma victims in the 1999 Marmara, Turkey earthquake. J Pediatr Surg. 2001; 36: 368–72. 10.3402/gha.v4i0.7196.
- WHO. Best practice guidelines on emergency surgical care in disaster situations. In: Best practice guidelines in disaster situations. Geneva: 2007.
- Emami MJ, Tavakoli AR, Alemzadeh H, Abdinejad F, Shahcheraghi G, Erfani MA, et al.. Strategies in evaluation and management of Bam earthquake victims. Prehosp Disaster Med. 2005; 20: 327–30.
- WHO. WHO manual of surgical care at the district hospital (SCDH). In: Integrated management for emergency and essential surgical care (IMEESC) tool kit: disaster management guidelines. Geneva: 2005. Available from: http://www.who.int/surgery/publications/imeesc/en/index.html.
- PAHO. Establishing a mass casualty management system. WashingtonDC: Pan American Health Organization. 2001. Available from: http://www.paho.org/english/ped/masscas.pdf.
- Cooper D. Mass casualty management in disasters. In: WHO: Health Action in Crisis. Geneva: World Health Organization. 2006. Available from: http://www.who.int/hac/events/experts2006/D_Cooper_Mass_casualth_disasters.pdf.
- Osaki Y, Minowa M. Factors associated with earthquake deaths in the great Hanshin-Awaji earthquake, 1995. Am J Epidemiol. 2001; 153: 153–6. 10.3402/gha.v4i0.7196.
- Naghi T, Kiani K, Mazlouman S, Taheri A, Kamrani R, Panjhavi B, et al.. Musculoskeletal injuries associated with earthquake. A report of injuries of Iran's December 26, 2003 Bam earthquake casualties managed in tertiary referral centers. Injury. 2005; 36: 27–32. 10.3402/gha.v4i0.7196.
- Bar-Dayan Y, Mankuta D, Wolf Y, Levy Y, Vanrooyen M, Beard P, et al.. An earthquake disaster in Turkey: an overview of the experiences of the Israeli Defense Forces Field Hospital in Adapazari. Disasters. 2000; 24: 262–70. 10.3402/gha.v4i0.7196.
- Armenian HK, Melkonian AK, Hovanesian AP. Long term mortality and morbidity related to degree of damage following the 1998 earthquake in Armenia. Am J Epidemiol. 1998; 148: 1077–84.
- Ramirez M, Peek-Asa C. Epidemiology of traumatic injuries from earthquakes. Epidemiol Rev. 2005; 27: 47–55. 10.3402/gha.v4i0.7196.
- Vanholder R, van der Tol A, De Smet M, Hoste E, Koc M, Hussain A, et al.. Earthquakes and crush syndrome casualties: lessons learned from the Kashmir disaster. Kidney Int. 2007; 71: 17–23. 10.3402/gha.v4i0.7196.
- The Sphere Project. Humanitarian charter and minimum standards in humanitarian response. Rugby: The Sphere Project. 2011. Available from: http://www.sphereproject.org/content/view/720/200/lang,english.
