
Abstract
Background
Behaviour is guided by perceptions and traditions. As such, understanding culture and religion is important in order to understand healthcare behaviour. Religious perceptions shape a person's understanding of the world and are maintained through texts and tradition. One such important religious text in relation to sexual and reproductive health is the Nativity story. This account of the conception and birth of Jesus is well known in the Christian cultural sphere and beyond, and it has for generations shaped perceptions of childbirth.
Methods
This paper attempts a re-reading of the Nativity story using a hermeneutic approach.
Results and Conclusion
This reveals a dual understanding of the Nativity, not just as an account of immaculate transcendence and a rosy Christmas tale, but as a source of identification for pregnant women and mothers and a call to action for improved maternal and child healthcare.
Introduction
Ideas shape our minds and our minds shape our behaviour (Citation1). Concepts of what is appropriate or right guide the way we do things (Citation2). Thus, tradition and ‘how we have always done things’ can become great barriers to the introduction of evidence-based practice (Citation3, Citation4). This tendency is particularly evident in maternal and child healthcare. The family, and reproduction, are central concepts around which we arrange our lives, and the surrounding structures are well guarded by tradition. Sexual relations, marriage, childbearing, birth, and the rearing and place of children are, in all cultures, heavily regulated to guide our relations and behaviour (Citation5). The cultural rules and traditions surrounding maternal and child health have been developed throughout history to protect humankind from internal and external threats. For example, the 1-month seclusion after delivery for mother and newborn, which is so common in many cultures, is aimed at protecting the neonate from infection. Today, however, we have new knowledge, and antibiotics to cure early childhood infections as well as home visits by healthcare workers to detect and act upon warning signs of infection. All of these interventions help to save a large proportion of the newborns who would otherwise die (Citation6). Cultural traditions and misconceptions can thus stand in the way of recent evidence that challenges how things are done, and they can be an obstacle to implementing positive behavioural change (Citation7, Citation8). Maternal and child health practitioners and researchers therefore need to address not only the medical side of the challenge, but also to obtain a deeper understanding of the cultural and contextual factors guiding end receivers’ behaviour.
Religion plays a vital part in bringing sense and meaning to reality (Citation1). All humans, from atheists to fundamentalist Buddhists, are guided in their behaviour by their perceptions and explanatory models of reality (Citation1). There is also a strong link between religion and health, an aspect that is many times neglected in healthcare research and delivery (Citation9). Major life course events such as birth, becoming a parent, and raising a child are all surrounded by rules and regulations derived from our religious and cultural thought patterns (Citation7, Citation8). To preserve these thought constructs, most religions have texts, sacred or traditional, to outline and encompass their messages and ideas. Even in oral traditions, repetition and preservation of the inherited storyline are essential elements (Citation2). The text is a sustaining force, a point of reference for religion's power of explanation. As such, religious texts create normalcy and can consequently be an important key to understanding behaviour (Citation2). One such text in the Christian tradition is the Nativity story, narrating the birth of Jesus. In the Christian tradition the Nativity story serves as the statement of Mary's virgin birth and Jesus’ subsequently immaculate nature, proclaiming Jesus as the Son of God (Citation10). As such, the Nativity is central to the theological message of Christianity. However, the story can also be, and has been, read as a story of a regular birth, stating and advocating for the humanity of Jesus, showing how the Son of God is also subject to normal human hardship (Citation10). In this capacity the Nativity story has become a popular folk tale, shaping perceptions of pregnancy and childbirth. Given the spread of this account of childbirth and the authority it has as a religious text, it is important to critically examine the text in the light of what we know and advocate for today in global maternal and child health. The aim of this paper is to apply a hermeneutic approach to the Nativity story, as it is portrayed in the Gospel of Luke.
Methods
Hermeneutics – contextual interpretation
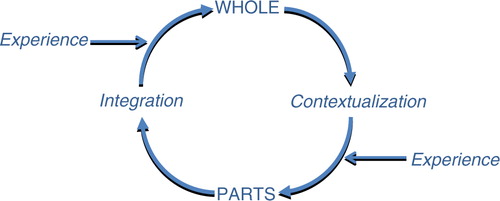
Hermeneutics can be described as the interpretation of text; it is a research methodology that departs from what is currently known. There are many schools and adaptations of hermeneutics, but basically hermeneutics set up rules for interpretation. By various means hermeneutic methods strive to create a deeper understanding and gain new insights by moving from the whole to the details and back to the whole, with input of experience and contextual interpretations along the way () (Citation11). The pre-understanding of a text, phenomenon, or cultural expression therefore has an important role in hermeneutics, as there is no objective starting point in relation to a text. The pre-understanding leads to understanding, which in turn becomes the new pre-understanding, and the hermeneutic circle is thus closed. Experience and new knowledge have an important role to feed into the hermeneutic circle and thereby fuel the process of a deeper and sometimes different understanding () (Citation11).
Fig. 1 The hermeneutic circle of interpretation.
Results
A religious success story
The Nativity story is many times perceived as something of a religious success story, an account of an immaculate birth, with angels singing and the whole of creation celebrating the birth of its saviour (Citation10). The account from the Gospel of Luke is read in churches and homes all over the world at Christmastime. Mary, the mother of Jesus, is perceived as a model of virtue, with a serving spirit, being the chosen one for the glorious mission of carrying the Son of God in her womb (Citation12). In many churches, especially within Catholicism, the Virgin Mary has an uplifted and celebrated position, not far removed from Jesus himself. This elevated status comes from an interpretation of the Nativity story as something of grandeur, with Mary as its main heroine (Citation12). In this way the pregnancy and childbirth of Mary becomes a role model account, not only shaping normality but also depicting the perfect.
An unwanted pregnancy
The hermeneutic approach now directs us to go from the whole, as described in the previous paragraph, to look more closely at the details (). This is done with the contextual addition of today's global maternal and child health. The first thing that can be noted is that the story begins with an unwanted pregnancy, a major challenge in maternal and child health. The message the angel delivers in Luke 1:31 is not only unexpected, but must in today's terms also be considered an unwanted pregnancy. Mary however does not protest by claiming the right to her own body, but succumbs to patriarchal authority (Luke 1:38). Angels in the Bible are usually men, and the response of Mary, to internalize the unexpected news of pregnancy and ‘hide it in her heart’, is a common strategy among many young women who cannot exercise the right over their own bodies. The unwanted pregnancy is not only stressful because of the biological changes that come with it, but also because of the high level of stigma associated with it. To be found pregnant out of wedlock was considered a crime in the Jewish culture of the time, and the penalty was death by stoning. Joseph, who was engaged to Mary, wanted to avoid the shame of having his betrothed being impregnated by another man. According to the gospel it took divine intervention for him to change his mind (Matthew 1:20). Mary subsequently decides to leave her hometown and travel to her older relative, Elizabeth (Luke 1:39–45). Most likely this was to conceal the pregnancy and avoid the associated stigma until it was undeniable. Mary stayed away for the first full trimester, thus avoiding pressure by family members and society at large to have an abortion, which may very well have been an option at the time. The situation many women find themselves in today is very similar (Citation13). It is quite possible that Mary planned to stay at her relative's house until the baby was born. This strategy remains quite common in unwanted pregnancies today and creates an unsafe environment for the newborn even before birth.
An unsafe delivery
The rest of the pregnancy seems to have been without complications and the next part of the Nativity story describes the delivery. It is preceded by a long and arduous journey, from Nazareth to Bethlehem (Luke 2:4–5), a trip of about 120 kilometres. Lack of rest and hard physical exertion are known risk factors for preterm birth. This might also be the reason for the poor birth preparations made by the two parents, resulting in Mary having to give birth in a stable (Luke 2:7). There is furthermore no account of any assistance at the birth, except maybe from Joseph. The delivery can hardly be considered to have been hygienic as the newborn was placed in a feeding trough for animals (Luke 2:7). Whether Mary initiated breastfeeding within one hour or not, as is the standard recommendation today, is not mentioned in the text, but it seems that skin-to-skin care was not practised. The gospel mentions explicitly that the newborn was ‘wrapped in cloths’ (Luke 2:12), indicating that this was the preferred method of the day. The account of Jesus’ birth thus contains many examples of unfavourable birth conditions, as outlined in .
Table 1 Observed reproductive health problems in the Nativity story
A problem catalogue
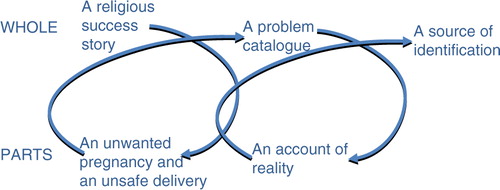
When we now continue in the hermeneutic circle we find that the Nativity story is far from a success story (). It is filled with public health risks and the picture that emerges is one of vulnerability and distress. Societal rules and regulations surrounding reproduction often cause problems when a pregnancy does not follow the accepted pattern, resulting in stigma and shame (Citation5). Mary is forced to choose to leave her home or to suffer disdain from her neighbours and even possible death for her and/or her unborn child. In addition, the delivery as a whole is filled with hardship and challenges and serves as more or less a catalogue of things to avoid for a healthy delivery. Lack of birth preparations, skilled assistance at birth, and proper postnatal care create far less than the perfect delivery situation. We can hence conclude that one lap in the hermeneutic circle leaves us with a completely different perception of the Nativity story.
Fig. 2 Hermeneutic interpretation of the Nativity story.
An account of reality
However, let us take another turn in the analysis and look at the parts in the light of today's global maternal and child health situation (). Millions of women still deliver without skilled assistance at birth and there is a great challenge in the implementation of high quality postnatal care (Citation14). Almost three million newborns die every year during the first 4 weeks of life (Citation14), despite existing evidence that simple interventions such as skin-to-skin care, early initiation of breast feeding, kangaroo mother care, and neonatal resuscitation could save the larger part of these newborn babies (Citation6, Citation15) (Citation16). The maternal and neonatal health problems identified in the Nativity story are consequently not unlike the current situation. At the time of Jesus’ birth these conditions would have been commonplace. In addition, the issue of unwanted pregnancies, which is a major public health challenge given that the unmet need for family planning is still high and there is little or no access to safe abortion methods, was probably a frequent problem at the time of Mary.
A source of identification
The picture that emerges after a second round in the hermeneutic circle is a rather blunt and straightforward description of the vulnerable situation of pregnancy and childbirth still experienced by many women today. Far from being a rosy account with heavenly hosts and adoring shepherds, the Nativity story depicts a number of problems addressed in the continuum of care. It thus becomes a source of identification rather than a testimony of immaculate transcendence. Maybe it is there the strength of the story lies, in the tension between reality and divinity? Mary has become an almost divine figure, worshipped by millions the world over, while at the same time being subject to many of the same conditions still faced by so many women today.
Discussion
A preserving force or a call to action?
Religious texts shape our perceptions of the world, not only in relation to the divine, but also by making sense of reality through establishing standards and norms for behaviour (Citation2). We have shown that a very well-known and influential religious text like the Nativity story can be interpreted in different ways depending on which perspective is applied. To overcome barriers to good health it is important to get a deeper understanding of underlying ideas and thought patterns that shape behaviour (Citation7, Citation9). Ideas of normality can many times prevent patients from seeking adequate care and may influence the level of empowerment in individuals. What is considered normal can be a source of resilience, but also a barrier for the acquisition or implementation of new knowledge. As a modelling benchmark, the Nativity story becomes a preserving force, maintaining misconceptions and harmful behaviours in relation to pregnancy and childbirth. On the other hand, the Nativity story supplies a description of reality with which many women can identify and thereby invokes a feeling of community that can spur action. To see that you are not alone, that even the Mother of God suffered suboptimal pregnancy and delivery care, subject to restricting cultural norms, can be a motivation to demand change. As such, the Nativity story becomes a call to action!
Authors' contributions
MM conceptualized, carried out and finalized the study.
Acknowledgements
This paper is written as part of the Network on Sexual and Reproductive Health (SRH), Gender and Religion, a collaboration between the Church of Sweden, Ethiopian Graduate School of Theology (EGST), Stellenbosch University, the University of KwaZulu-Natal in South Africa, and Tumaini University in Makumira, Tanzania. The network is supported by the Church of Sweden and the Swedish International Development Cooperation Agency. The author is a medical doctor by profession, currently working for the Church of Sweden within a health outreach project in Swaziland. The author acknowledges Dr Adamo Addissie of EGST for inspiration in the conceptualization of the paper and Ruth Newman for language editing.
Conflict of interest and funding
The author has not received any funding or benefits from industry or elsewhere to conduct this study. The author declares no conflict of interest.
References
- Ellison CG, Levin JS. The religion-health connection: evidence, theory, and future directions. Health Educ Behav. 1998; 25: 700–20.
- Evola V. Cognitive semiotics and on-line reading of religious texts. Conscious Lit Arts. 2005; , pp. 44–66
- Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care. 1998; 7: 149–58.
- Santesso N, Tugwell P. Knowledge translation in developing countries. J Contin Educ Health Prof. 2006; 26: 87–96.
- Cook RJ, Dickens BM. Reducing stigma in reproductive health. Int J Gynaecol Obstet. 2014; 125: 89–92.
- Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N, de Bernis L. Evidence-based, cost-effective interventions: how many newborn babies can we save?. Lancet. 2005; 365: 977–88.
- Gonnerman MEJr., Lutz GM, Yehieli M, Meisinger BK. Religion and health connection: a study of African American, Protestant Christians. J Health Care Poor Underserved. 2008; 19: 193–9.
- UNICEF, Collaborating Centre for Operational Research and Evidence. Apostolic religion, health and utilization of maternal and child health services in Zimbabwe. 2011; Harare: The United Nations Children's Fund.
- Levin JS. How religion influences morbidity and health: reflections on natural history, salutogenesis and host resistance. Soc Sci Med. 1996; 43: 849–64.
- Aichele G. Simulating Jesus: reality effects in the Gospels. 2015; New York: Routledge.
- Bontekoe R. Dimensions of the hermeneutic circle. 1996; Atlantic Highlands, NJ: Humanities Press International.
- Mellon J. The Virgin Mary in the perception of women. 2008; Jefferson, NC: McFarland.
- Olsson P, Wijewardena K. Unmarried women's decisions on pregnancy termination: qualitative interviews in Colombo, Sri Lanka. Sex Reprod Healthcare. 2010; 1: 135–41.
- Sharma G, Mathai M, Dickson KE, Weeks A, Hofmeyr G, Lavender T, etal. Quality care during labour and birth: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015; 15(Suppl 2): S2.
- Enweronu-Laryea C, Dickson KE, Moxon SG, Simen-Kapeu A, Nyange C, Niermeyer S, etal. Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015; 15(Suppl 2): S4.
- Haws RA, Thomas AL, Bhutta ZA, Darmstadt GL. Impact of packaged interventions on neonatal health: a review of the evidence. Health Policy Plan. 2007; 22: 193–215.