Abstract
Background
In a situation where national censuses do not record information on ethnicity, studies of the indigenous Sámi people's health and living conditions tend to use varying Sámi inclusion criteria and categorizations. Consequently, the basis on which Sámi study participants are included and categorized when Sámi health and living conditions are explored and compared differs. This may influence the results and conclusions drawn.
Objective
To explore some numerical consequences of applying principles derived from Norway's Sámi Act as a foundation for formalized inclusion criteria in population-based Sámi studies in Norway.
Design
We established 1 geographically based (G1) and 3 individual-based Sámi example populations (I1–I3) by applying diverse Sámi inclusion criteria to data from 17 rural municipalities in Norway north of the Arctic Circle. The data were collected for a population-based study of health and living conditions in 2003–2004 (the SAMINOR study). Our sample consisted of 14,797 participants aged 36–79 years.
Results
The size of the individual-based populations varied significantly. I1 (linguistic connection Sámi) made up 35.5% of the sample, I2 (self-identified Sámi) made up 21.0% and I3 (active language Sámi) 17.7%. They were also noticeably unevenly distributed between the 5 Sámi regions defined for this study. The differences for the other characteristics studied were more ambiguous. For the population G1 (residents in the Sámi language area) the only significant difference found between the Sámi and the corresponding non-Sámi population was for household income (OR=0.69, 95% CI: 0.63–0.74). For the populations I1–I3 there were significant differences on all measures except for I2 and education (OR=1.09, 95% CI: 0.99–1.21).
Conclusions
The choice of Sámi inclusion criterion had a clear impact on the size and geographical distribution of the defined populations but lesser influence on the selected characteristics for the Sámi populations relative to the respective non-Sámi ones.
Most of the indigenous Sámi people's traditional settlement area, Sápmi, corresponds to the central and northern parts of Norway, Sweden and Finland; a small portion covers the Kola Peninsula in north-western Russia. Studies of Sámi health and living conditions tend to use a variety of Sámi inclusion criteria and Sámi-internal categorizations (Citation1–Citation7). This may lead to uncertainty when the Sámi people's health and living conditions are studied and compared externally, internally, and over time.
Conceptually, indigenous peoples are also ethnic groups (Citation8). Ethnicity is a complex phenomenon and it is not clear how and to what degree ethnicity is related to health (Citation9, Citation10). There is also uncertainty as to the appropriate, available and ethically acceptable procedures for obtaining the data needed to study health and ethnicity in interplay (Citation11–Citation16). Nevertheless, any study that relates to ethnically defined subpopulations must identify the groups in question. Thus, understandings and operationalizations of ethnicity as well as availability of relevant ethnicity data are crucial when designing population-based studies of indigenous people's health and living conditions.
A recent global survey found that 63% of all countries included some kind of “ethnic information” in their national censuses (Citation17). This practice is thus widespread but not obvious. In the countries dividing Sápmi, there are various practices in time and space. For example, until 1930 many Norwegian and Swedish censuses did, in various ways and with various designations, identify Sámi citizens; after 1945 this has only happened as a few geographically limited exceptions (Citation18–Citation20). Despite some inter-country variations, the present situation is a fundamental lack of systematic up-to-date Sámi demographic data. A part of this situation is, however, that the Sápmi area historically has been the home of several ethnic groups. Although there have been hierarchies in terms of power and status, including periods of forced assimilation of the Sámi, the various groups have also interacted (Citation21–Citation23). The foundation for Sámi ethnicity and the basis for individuals’ self-identification as Sámi is thus ambiguous. Hence, even if information on Sámi affiliation had been systematically collected in official contexts, it is not given which persons could and would have been recorded as Sámi.
An absence of ethnicity data in national censuses implies that official ethnic categories are also absent. However, in Norway a special Sámi Act passed in 1987 has stated some criteria for the right to participate in elections to a national Sámi representative body – the Sámediggi in Northern Sámi. The act also states the right to use Sámi language in certain contexts. In this study, we wanted to explore the possibility of utilizing principles derived from this act as a foundation for formalized inclusion criteria in Sámi population-based studies in Norway. The aim was to define Sámi example populations based on these principles and to present some numerical consequences of this. We also aimed to determine whether different definitions would provide different effects when the outcomes on 3 measures related to health and living conditions were compared for each corresponding Sámi and non-Sámi population.
Materials and methods
Data and study population
We used data collected in 2003–2004 for the SAMINOR study, a population-based cross-sectional study of health and living conditions in selected rural and semi-rural areas in the Norwegian part of Sápmi, where available knowledge indicated the presence of some Sámi population (Citation24). The SAMINOR study was initiated by the Centre for Sámi Health Research at the University of Tromsø and was conducted in collaboration with the Norwegian Institute of Public Health. The study included 24 municipalities, 18 north of and 6 south of the Arctic Circle. In 7 municipalities, the study was however limited to certain villages ().
Fig. 1. Municipalities included in the SAMINOR study.
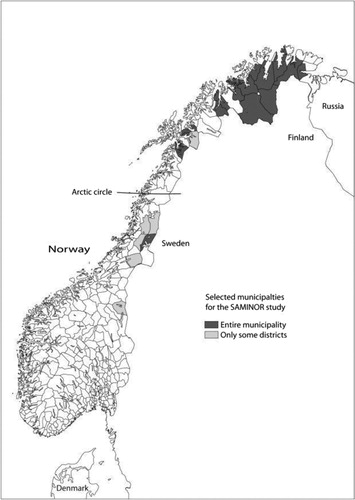
In total 27,987 persons living in the selected areas, aged 36–79 years, were invited to participate. Among these, 60.6% returned at least one of the study's three questionnaires. Our study included 14,797 participants aged 36–79 years who (a) were resident north of the Arctic Circle in 1 of the 17 entirely involved municipalities, and (b) had returned the questionnaire including the questions about ethnicity. As of 1 January 2003, the total population in our study area amounted to 1.1% of Norway's total population.
Sámi example populations
We defined a set of Sámi populations based on principles derived from the Sámi Act) (Citation25). This act states that the Sámi in Norway shall have a nationwide Sámi representative body, elected by and among those Sámi who have joined a separate electoral roll established for this purpose. The right to enrol requires that a person declares to fulfil both a subjective criterion of self-identification as Sámi and an objective criterion saying that the person or at least 1 parent, grandparent or great-grandparent has or has had Sámi as a language at home, or that the person is the child of an enrolled person (Section 2-3). Since 1990 the Sámi Act has given individuals the right to use Sámi language in certain contexts, primarily in municipalities designated as the Sámi Language Administrative District (Section 3-1). This area – hereafter the Language Area – originally comprised 6 municipalities, but has, since 2006, gradually been extended to 10, 8 of which are in our study area.
There appear to be 2 premises to be derived from the Sámi Act: that Sámi identification shall be self-ascribed, and that the Sámi language has a particular status as a basis for Sámi rights. The latter relates to geography (cf. the Language Area) and to the individual – to persons who speak Sámi (cf. the right to use the Sámi language) and to persons whom this was the case for at least 1 person in the 3 previous generations (cf. the objective criterion for enrolment in the Sámediggi electoral roll). We synthesized the 2 premises into 3 principles which we considered to be a salient basis for defining Sámi populations, namely (a) geographical location, (b) linguistic connection and (c) ethnic self-identification.
The SAMINOR study was conducted in municipalities with a minimum proportion of Sámi residents. The entire study sample might thus be regarded as a kind of geographically based Sámi population (G0). However, with reference to the Sámi Act, we defined 4 more or less overlapping Sámi populations: 1 geographically based (G1) and 3 individual-based (I1–I3). The geographical population G1 consists of all participants resident in the municipalities included in the Language Area in 2013. In our study area these are Nesseby, Tana, Porsanger, Karasjok, Kautokeino, Kåfjord, Lavangen and Tysfjord – listed from northeast towards south, Norwegian names only. The participants’ geographical affiliation was stated in address data obtained from the Norwegian National Population Register.
Two individual-based Sámi populations, I1 and I2, were defined with reference to the objective and the subjective criterion for enrolment in the Sámediggi electoral roll. Population I1 consists of individuals who reported any kind of Sámi linguistic connection in 3 generations (the criterion in the Sámi Act also includes great-grandparents’ language, but our data only cover 3 generations). Population I2 consists of those who reported self-identification as Sámi. A third individual-based population I3 is composed of those who reported Sámi as an active language. Assignment to I1–I3 was based on self-reported replies to the 2 SAMINOR questions (a) What language do or did you, your parents, and your grandparents use at home? and (b) What do you consider yourself? For all questions, one or more boxes could be ticked for the options “Norwegian,” “Sámi,” “Kven” and “Other, please describe” (in our study area “Kven” represents descendants of Finnish pre-1945 immigrants, now formally recognized as a national minority in Norway). The responses about language were to be specified for each parent and grandparent. We categorized the person/language as Sámi when the Sámi option was ticked, either alone or combined with one or more other options.
We also defined 2 non-Sámi populations (N0 and N1) consisting of participants who had not ticked the Sámi option for any of these questions. Population N0 covers those in the entire study area whereas N1 are restricted to those in the Language Area. The non-Sámi thus does not constitute an ethnic group but represent statistical populations compiled for analytical purposes.
Demographic variables
We used data on gender and age provided by the Norwegian Central Population Register. We divided the variable “Age” into the categories “36–48 years,” “49–61 years” and “62–79 years.” To obtain a more detailed picture of each population's geographical distribution, we constructed the variable “Region” where the 17 municipalities were grouped into 5 regions, based primarily on Sámi cultural distinctions but also on location and population size ().
Fig. 2. Sámi regions defined for this study*. *Detailed Region labels: 1, Inner Language Area (2 municipalities); 2, Outer Language Area (4 municipalities); 3, Areas of Northern Troms/Finnmark (6 municipalities); 4, Alta municipality; 5, Areas of Nordland/Southern Troms (4 municipalities). The 6 municipalities in Region 1 and 2 together with 2 of those in Region 5 (the southernmost and the northernmost) make up those 8 municipalities in the Sámi Language Administrative District in 2013 that are included in our study area.
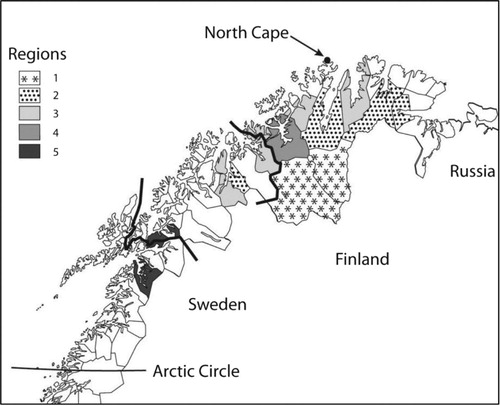
Six municipalities that make up the original Language Area constitute Region 1 'Inner Language Area’ (Kautokeino and Karasjok) and Region 2 'Outer Language Area’ (Kåfjord, Porsanger, Tana and Nesseby). This distinction was made because the Sámi language during recent decades has had a stronger position in the 2 municipalities of Region 1. Six municipalities with traditional coastal Sámi settlement constitute Region 3 'Areas of Northern Troms/Finnmark’ (Storfjord, Lyngen, Kvænangen, Loppa, Kvalsund and Lebesby). Region 4 ‘Alta’ covers only 1 municipality, Alta, which is also on the coast but because of a large and expanding population declared town status in 2000. Region 5 'Areas of Nordland/Southern Troms’ consists of 4 municipalities with Lule Sámi (Tysfjord) and Marka (i.e. outlying fields in the inland area) Sámi settlements (Evenes, Skånland and Lavangen). Tysfjord and Lavangen were included in the Language Area in 2006 and 2009, respectively.
Measures related to health and living conditions
We used SAMINOR questions to construct 3 measures widely used in studies of health and living conditions, namely education, household income and self-reported health. “How many years of education have you completed?” was divided into the categories “less than 12 years” and “more than 12 years,” corresponding to maximum completed high school and minimum commenced higher education, respectively. “How big is the family/household gross income per year?” had originally 6 response categories, but we constructed a dichotomous variable “Household income” with a cut-off point at 300,000 NOK. “Self-rated health” was dichotomized into “good” and “not good,” based on “How is your health now?”, which originally had 4 options.
Statistical analyses
Statistical analyses were performed in STATA, Version 12. Frequency tables were used for descriptive analyses. Logistic regression was used to compare (dichotomized) outcomes for the 3 measures related to health and living conditions for each Sámi and the corresponding non-Sámi population defined by the various Sámi inclusion criteria.
Ethics
The SAMINOR study was approved by the Regional Ethics Committee for Medical Research in Northern Norway. A Sámi consultant participated in the review of the application. Permission for retention of personal data was provided by the Norwegian Data Inspectorate. Beyond this, in contrast to many other indigenous peoples, the Sámi have not adopted Sámi-specific guidelines or procedures for research involving Sámi participants (Citation26).
Results
Table presents the absolute and relative size of the defined populations. Those with Sámi linguistic connection were twice as many as those reporting Sámi as the active language. The number of self-identified Sámi was somewhat higher than that of active-language users. Additional calculations show that among linguistic connection, 59.3% reported Sámi self-identification and 49.8% reported Sámi as the active language. Among the self-identified Sámi 83.9% reported being a Sámi speaker. Those residents inside the Language Area and with negative reporting on all Sámi inclusion criteria made up 39.1% of all respondents in this area. gives a schematic illustration of the 4 defined Sámi populations.
Fig. 3. Schematic illustration of 4 Sámi populations aged 36–79 years as of 2003–2004 in 17 municipalities in Norway north of the Arctic Circle – defined according to different but partially overlapping Sámi inclusion criteria*. *The size and relative position of each circle is indicative. Assignment to I1–I3 is based on self-reported data.
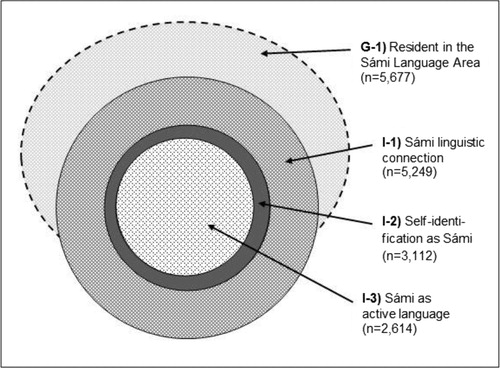
Table I Five Sámi and 2 non-Sámi populations aged 36–79 years as of 2003–2004 in 17 municipalities in Norway north of the Arctic Circle – defined according to different but partially overlapping Sámi inclusion/exclusion criteria*
Characteristics of the 5 Sámi populations are shown in Table . The gender and age distributions were fairly uniform, but those with Sámi as the active language had a slightly higher proportion of the oldest category at the expense of the youngest.
Table II Distribution of characteristics of 5 Sámi populations aged 36–79 years per 2003–2004 in 17 municipalities in Norway north of the Arctic Circle – defined according to different but partially overlapping Sámi inclusion criteria
The geographical variations were far more striking. The linguistic connection-based population was the only one with the largest share settled in Region 2 Outer language area. This population was also somewhat lesser unevenly distributed than the 2 other individual-based populations, whose patterns of regional distribution were fairly similar. In the population defined according to Sámi as the active language, 83.1% was resident in Region 1 or Region 2, the inner and the outer Language area.
With respect to household income, the proportion having the most favourable outcome sank gradually from 61.4 to 50.0% along the “population axis” G0–I3. Similar trends were revealed for education and self-rated health but with smaller relative differences. However, for education the pattern was broken by the self-identified Sámi having the largest proportion with the better outcome.
Characteristics of the 2 non-Sámi populations (Table ) had similar patterns to those of the 2 geographically based populations, respectively (cf. Table ). The geographical variations were, however, even greater and for household income the non-Sámi populations had a slightly larger proportion of those with the better outcome.
Table III Distribution of characteristics of 2 non-Sámi populations aged 36–79 years as of 2003/2004 in 17 municipalities in Norway north of the Arctic Circle – defined according to not having reported self-identification as Sámi or Sámi linguistic connection within 3 generations*
Table presents odds ratios (OR) and 95% confidence interval (CI) for education, household income and self-rated health for each of the populations G1 and I1–I3. The respective OR and CI are calculated by using as reference group each population's respective non-Sámi proportion of the study sample. All measures are adjusted for gender and age. For household income, the members of all the defined Sámi populations had significant – and markedly – lower odds for better outcome than the respective non-Sámi populations. Also self-rated health displayed a less favourable result for the 4 Sámi populations. The finding was however not significant for the population comprising all those in the Language Area (OR=0.98, CI: 0.91–1.06). The most diverse findings were those concerning the odds of having higher education. Whereas definitions based on Sámi linguistic connection and Sámi as the active language resulted in lower odds for Sámi versus non-Sámi, there was no significant difference between Sámi and non-Sámi population when using the definition based on geography, that is, all in the Language Area (OR 0.96 and CI 0.89–1.05) and the definition based on self-identification as Sámi (OR 1.09 and CI 0.99–1.21).
Table IV Adjusted odds ratio (OR) and 95% confidence interval (CI) for education, household income and self-rated health when 4 partially overlapping Sámi populations aged 36–79 years as of 2003–2004 in 17 municipalities in Norway north of the Arctic Circle are related to each population's respective non-Sámi proportion of the study sample*
When testing the heterogeneity of the individual-based Sámi inclusion criteria separately (I1–I3, cf. Table ), we found statistically significant difference only for education between self-identified Sámi and the 2 other populations respectively, whereas heterogeneity testing including the geographically defined population (G1) revealed a higher degree of heterogeneity between the different populations (data not shown).
Discussion
We found that the size and geographical distribution of a Sámi study population were noticeably affected by Sámi inclusion criterion. The differences for the other characteristics studied were more varied. A proportion of about 40% self-reported non-Sámi in the Language Area is also noteworthy. The findings must be viewed in light of Norway's assimilation policy, the so-called Norwegianization. From about 1850 to about 1950–1980, depending on the definition, this policy entailed a systematic governmental effort to make Sámi give up their language, change the basic values of their culture and replace their Sámi identity (Citation23). The policy was by and large successful; many who could have been Sámi speakers and/or self-identified as Sámi did gradually loose or drop these identification markers, particularly in coastal areas (Citation27–Citation29).
Although the modern Sámi movement in Norway during the 1970s led to a gradual change towards the objective that no one (any longer) should deny, conceal or give up Sámi identity and language (Citation30), the historical legacy of the Norwegianization is still manifest. This is demonstrated by the fact that self-identified Sámi in this study was equivalent to about 60% of linguistic connection Sámi. But while not self-identifying as Sámi despite having a Sámi linguistic connection might indicate that Sáminess (still) carries a social stigma, in some communities more than others, it is also widely agreed upon that ethnicity and ethnic affiliation are complex phenomenons which over time have been understood and dealt with differently by both scholars and laymen. Thus, to not self-identify as Sámi might for some individuals be based on rational assessment; they could have been Sámi, but do not consider themselves as such because their way of living does not coincide with their understanding of “what it means to be Sámi” (Citation31–Citation37). Their “objective” Sámi connection does anyway persist.
Those who reported Sámi as active language made up the smallest population. However, this group might be of particular interest – with respect to linguistic accommodation of health services for the Sámi-speaking population in a specific area and also, to studies of this topic. Besides, to define the speakers of Sámi language as a distinct population takes into account the possibility of being a Sámi speaker without having Sámi ancestry.
Whereas the use of individual-based Sámi inclusion criteria requires access to self-reported data, the use of geographical criteria is more straightforward. Pragmatically this might be a tempting alternative since much data can be obtained from regular municipality statistics. However, analyses and interpretations must take into account that a geographically defined Sámi population inevitably will have a non-Sámi share; in our study 39.1% in the Language Area. Also, the use of geographical criteria excludes the experiences of Sámi who live in communities with less Sámi-ethnic density, in itself a matter of interest.
Studies combining ethnicity and health-related issues do often have between-group equality and equity as focal aspects. In our study the geographical definition of a Sámi population implied a significant difference between Sámi and non-Sámi populations for household income only. The individual-based definitions resulted in significant differences on all measures except on education for self-identified Sámi. The significant differences were all to the disadvantage of the Sámi, though only to a minor extent with respect to education and self-rated health. However, while between-group differences clearly are of interest for Sámi and other indigenous peoples, it is also essential to have knowledge of each indigenous people's health and living conditions per se. Such knowledge is necessary as a means for the implementation of the principles in the UN Declaration on the rights of indigenous peoples (Citation38). This includes knowledge about within-group differences among Sámi; whether and how Sámi health varies with affiliation to various Sámi communities and also, with the belonging to other social groups than the ethnic one (Citation39).
Scholars have pointed out that studies of health and ethnicity tend to underestimate or under-communicate that ethnicity is context-dependent and invokes explicit and articulated operationalization in each case (Citation40–Citation42). In fact, failing to provide the context and definitions of study populations is claimed to be a common mistake in studies of health patterns at the population level (Citation43). This is problematic because it can affect the calculations of interest, the understanding of causal relationships, and also the potential for generalization (Citation44). Thus, when health studies include ethnic populations it is particularly important – and maybe also particularly challenging – to articulate the demographic frameworks and to specify the analytic categories. This is perhaps even more essential in studies involving indigenous peoples (Citation45–Citation47). Our study contributes to on-going efforts to deal with such challenges in a Sámi context.
We would argue that a key challenge for population-based Sámi studies is to manage the relationship between the inclusion criteria based on Sámi linguistic connection and self-identification as Sámi. One aspect is that these 2 populations differ in several respects, especially geographically. But it is also important that it seems to have become (ethically) preferable to base ethnicity data on self-identification (Citation48). For instance, the United Nations explicitly recommends self-identification when ethnicity is recorded in a national census, including also the possibility of multi-ethnic identification (Citation49). However, because some persons who do not (any longer) identify with a particular ethnic group still might be influenced by having a (former) connection to this group, it may be appropriate to combine “subjective” data based on self-identification with data based on one or more “objective” manifestations of ethnic affiliation, even though reporting of the latter may also be unstable. Dilemmas arising from incorporating and presenting individuals as something “other” than what they consider themselves to be should however be explicitly addressed.
Limitations
The Sámi data situation implies that it is not possible to assess whether there are ethnic biases in the sample. The self-reported Sámi ethnicity data must be related to that all SAMINOR participants were born before 1969 and thus might have life experiences affected more by the Norwegianization of the past than by the Sámi revitalization of more recent decades. We did not take into account that some respondents had ticked for more than one option when answering the ethnicity questions. Neither did we consider possible inconsistencies in the reporting.
Conclusion
Every population-based Sámi study, whether having a Sámi/non-Sámi “dichotomy perspective” or a Sámi-internal “gradient perspective”, has to decide on how to define participants as Sámi participants. Our pioneering exploration of the utilization of formalized Sámi inclusion criteria demonstrated that the choice of criterion affected the size and geographical distribution of the various Sámi populations. The impact of the criterion on the selected characteristics for each of the Sámi populations relative to the respective non-Sámi ones was small, though not absent. Generally speaking, however, any study of Sámi health and living conditions would benefit from a transparent assessment of utilizing formalized Sámi inclusion criteria.
Conflict of interest and funding
No competing interests. The study was funded by Norwegian Research Council and Sámi University College.
Acknowledgements
The authors acknowledge statistician Marita Melhus (UiT The Arctic University of Norway) for statistical advices and the making of the and . The authors would also acknowledge the statistical advice from statistician Tonje Braaten (UiT The Arctic University of Norway), Professor Nils Oskal (Sámi University College) for valuable discussions and inputs to our work, and Paul Farmer for language editing.
Related Research Data
References
- Silviken A, Kvernmo S. Suicide attempts among indigenous Sami adolescents and majority peers in Arctic Norway: prevalence and associated risk factors. J Adolesc. 2007; 30: 613–26.
- Brustad M, Pettersen T, Melhus M, Lund E. Mortality patterns in geographical areas with a high vs. low Sami population density in Arctic Norway. Scand J Publ Health. 2009; 5: 475–80.
- Bals M. Risk and protective factors associated with internalizing symptoms in Sami and non-Sami adolescents in Arctic Norway. [dissertation]. 2010; Tromsø: University of Tromsø.
- Hansen KL. Ethnic discrimination and bullying in relation to self-reported physical and mental health in Sami settlement areas in Norway. The Saminor study. [dissertation]. 2011; Tromsø: University of Tromsø.
- Hassler S, Sjölander P, Ericsson AJ, Lantto P, Sköld P. Construction of a database on health and living conditions of the Swedish Sami population. Befolkning och bosätting i norr. Etnicitet, identitet och gränser i historiens sken [Population and settlement in the north. Ethnicity, identity and borders in the light of history]. 2004; Umeå: Umeå Universitet. 127–24.
- Norum J, Nieder C. Socioeconomic characteristics and health outcomes in Sami speaking municipalities and a control group in northern Norway. IJCH. 2012; 71: 19127.
- Soininen L, Pokhrel A, Dyba T, Pukkala E, Hakulinen T. Survival of Sami cancer patients. IJCH. 2012; 71: 18959.
- Makkonen T. Identity, difference and otherness. The concepts of ‘people’, ‘indigenous people’ and ‘minority’ in international law. 2000; Helsinki: University of Helsinki, Faculty of Law.
- Bhopal R. Medicine and public health in a multiethnic world. J Public Health Med. 2009; 31: 315–21.
- Krieger N, Whitmarsh I, Jones DS. The science and epidemiology of racism and health: racial/ethnic categories, biological expressions of racism, and the embodiment of inequality – an ecosocial perspective. What's the use of race? Modern governance and the biology of difference. 2010; Cambridge, MA: MIT Press. 225–55.
- Smylie J, Anderson I, Ratima M, Crengle S, Anderson M. Indigenous health performance measurement systems in Canada, Australia, and New Zealand. Lancet. 2006; 367: 2029–31.
- Boyd KM. Ethnicity and the ethics of data linkage. BMC Public Health. 2007; 7: 317–9.
- Cormack D, Harris R. Issues in monitoring Māori health and ethnic disparities: an update. 2009; Wellington: Te Ro¯pū Rangahau Hauora a Eru Po¯mare.
- Varcoe C, Browne AJ, Wong S, Smye VL. Harms and benefits: Collecting ethnicity data in a clinical context. Soc Sci Med. 2009; 68: 1659–66.
- McGregor J. Racial, ethnic, and tribal classifications in biomedical research with biological and group harm. Am J Bioeth. 2010; 10: 23–4.
- Lofters AK, Shankardass K, Kirst M, Quinonez C. Sociodemographic data collection in healthcare settings. An examination of public opinions. Med Care. 2011; 49: 193–9.
- Morning A. Ethnic classification in global perspective: a cross-national survey of the 2000 census round. Popul Res Pol Rev. 2008; 27: 239–72.
- Lie E. Numbering the nationalities: ethnic minorities in Norwegian population censuses 1845–1930. Ethn Racial Stud. 2002; 25: 802–22.
- Axelsson P. Abandoning “the Other”: statistical enumeration of Swedish Sami, 1700 to 1945 and beyond. Ber Wissenschaftsgesch. 2010; 33: 263–79.
- Pettersen T, Axelsson P, Sköld P. Out of the backwater? Prospects for contemporary Sami demography in Norway. Indigenous peoples and demography: the complex relation between identity and statistics. 2011; Oxford: Berghahn. 185–96.
- Niemi E. Kategorienes etikk og minoriteter i nord. Et historisk perspektiv [The ethics of categorization and the minorities in the North. A historical perspective]. Samisk forskning og forskningsetikk [Sámi research and research ethics]. 2002; Oslo: Den nasjonale forskningsetiske komité for samfunnsvitenskap og humaniora. 22–44.
- Hansen LI, Olsen B. Samenes historie fram til 1750 [History of the Sámi to the year 1750]. 2004; Oslo: Cappelen Akademisk.
- Minde H. Assimilation of the Sami: implementation and consequences. 2005; Kautokeino: Galdu, Resource Centre for the Rights of Indigenous Peoples.
- Lund E, Melhus M, Hansen KL, Nystad T, Broderstad AR, Selmer R, etal. Population based study of health and social conditions in areas with both Sámi and Norwegian inhabitants – the SAMINOR study. IJCH. 2007; 66(2): 113–28.
- Act of 12 June 1987 No. 56 concerning the Sameting (the Sami parliament) and other Sami legal matters (the Sami Act). Translation of Lov om Sametinget og andre samiske rettsforhold (sameloven). Available from: http://www.regjeringen.no/en/doc/laws/Acts/the-sami-act-.html?id=449701.
- Porsanger J. Ethical conduct in research involving Indigenous peoples: general considerations. Ethics in Sámi and indigenous research/Sáme- ja álgoálbmotdutkama etihkka: seminára raporta, Kárášjohka. Diedut. 2008; Guovdageaidnu: Sámi Instituhtta. 24–36.
- Eidheim H. Aspects of the Lappish minority situation. 1971; Oslo: Universitetsforlaget.
- Nielsen R. Folk uten fortid [People without a past]. 1986; Oslo: Gyldendal.
- NOU. Om samenes rettsstilling [The legal position of the Sámi]. 1984; Oslo: Ministry of Justice. 18.
- Stordahl V, Eriksen TH. Samene: Fra “lavtstaaende race” til “urbefolkning” [The Sámi: From an “inferior race” to an “indigenous people”]. Flerkulturell forståelse [Multicultural understanding]. 1997; Oslo: Tano Aschehoug. 139–52.
- Høgmo A. Det tredje alternativ. Barns læring av identitetsforvaltning i samisk-norske samfunn preget av identitetsskifte [The third alternative. Children's learning of identity management in Sámi-Norwegian communities characterized by identity change]. Tidsskrift for samfunnsforskning. 1986; 395–416.
- Stordahl V. Same i den moderne verden. Endring og kontinuitet i et samisk lokalsamfunn [Sámi in the modern world. Change and continuity in a Sámi community]. 1996; Karasjok: Davvi Girji.
- Hegg L. Norsk eller samisk? I spenningsfeltet mellom eksistens og vitenskap [Norwegian or Sámi? In the field of tension between existence and science] [Master]. 2000; Tromsø: Universitetet i Tromsø.
- Andersen S, Bjerkli B, Selle P. Samisk tilhørighet i kyst- og fjordområder [Sámi affiliation in fjords and coastal areas]. Samer, makt og demokrati: Sametinget og den nye samiske offentligheten [Sámi, power and democracy. The Sámi Parliament and the new Sámi public sector]. 2003; Oslo: Gyldendal Akademisk. 246–64.
- Paine R, Bjerkli B, Selle P. Identititetsfloke same-same: om komplekse identitetsprosesser i samiske samfunn [The tangle of mutual Sámi identity: complex identity processes in Sámi communities]. Samer, makt og demokrati: Sametinget og den nye samiske offentligheten [Sámi, power and democracy. The Sámi Parliament and the new Sámi public sector]. 2003; Oslo: Gyldendal akademisk. 291–317.
- Thuen T, Bjerkli B, Selle P. Lokale diskurser om det samiske [Local discourses on Sámi matters]. Samer, makt og demokrati: Sametinget og den nye samiske offentligheten [Sámi, power and democracy. The Sámi Parliament and the new Sámi public sector]. 2003; Oslo: Gyldendal akademisk. 265–90.
- Olsen K. Identities, ethnicities and borderzones. Examples from Finnmark, Northern Norway. 2010; Stamsund: Orkana akademisk.
- Stavenhagen R, Charters C, Stavenhagen R. Making the declaration work. Making the declaration work: the United Nations declaration on the rights of indigenous peoples. 2009; Copenhagen: IWGIA. 352–71.
- Hankivsky O, de Leeuw S, Lee J-A, Vissandjée B, Khanlou N, Hankivsky O, de Leeuw S, Lee J-A, Vissandjée B, Khanlou N. Introduction: purpose, overview, and contribution. Health inequities in Canada: intersectional frameworks and practices. 2011; Vancouver: UBC Press. 1–15.
- Bradby H. Describing ethnicity in health research. Ethn Health. 2003; 8: 5–13.
- Ford CL, Harawa NT. A new conceptualization of ethnicity for social epidemiologic and health equity research. Soc Sci Med. 2010; 71: 251–8.
- Baer RD, Arteaga E, Dyer K, Eden A, Gross R, Helmy H, etal. Concepts of race and ethnicity among health researchers: patterns and implications. Ethn Health. 2013; 18: 211–25.
- Bhopal R. Seven mistakes and potential solutions in epidemiology, including a call for a World Council of Epidemiology and Causality. Emerg Themes Epidemiol. 2009; 6: 6.
- Bhopal R. Concepts of epidemiology: integrating the ideas, theories, principles and methods of epidemiology. 2008; 2nd ed, Oxford: Oxford University Press.
- Bartlett JG, Madariaga-Vignudo L, O'Neil JD, Kuhnlein HV. Identifying indigenous peoples for health research in a global context: a review of perspectives and challenges. IJCH. 2007; 66: 287–307.
- Simmonds S. The implications of using different methods to measure ethnicity in a cohort study. [dissertation]. 2010; Wellington: University of Otago.
- Kukutai T. The thin brown line: re-indigenizing inquality in Aotearoa New Zealand [dissertation]. 2010; Stanford: Stanford University.
- European Commission. European handbook on equality data: why and how to build to a national knowledge base on equality and discrimination on the grounds of racial and ethnic origin, religion and belief, disability, age and sexual orientation. 2007; Luxembourg: Office for Official Publications of the European Communities.
- United Nations. Principles and recommendations for population and housing censuses. 2008; New York: United Nations.