
Abstract
Introduction
For obvious reasons, athletes are at greater risk of sustaining a lumber (lower) spine injury due to physical activity. To our knowledge, no previous studies have examined the prevalence of low back pain (LBP) in a Tunisian sports and physical education institute.
Aim
To assess the prevalence of LBP in different sports among students studying in a sports and physical education institute in Tunisia, to determine the causes of the injuries, and to propose solutions.
Methods
A total of 3,379 boys and 2,579 girls were studied. A retrospective cross-sectional survey was conducted on a group of students aged 18.5–24.5 years at the Higher Institute of Sport and Physical Education of Sfax to estimate the prevalence of LBP and its relation to the type of sports. Data on age, weight, height, smoking, and the sport in which the student was injured in the low back were collected from the institute health service records from 2005 until 2013.
Results
LBP was reported by 879 of the 5,958 study participants (14.8%). The prevalence of LBP was significantly higher (p<0.001) in females (17.6%) than in males (12.5%). LBP prevalence did not differ by body mass index or smoking habit (p>0.05). The sports associated with the higher rates of LBP were gymnastics, judo, handball, and volleyball, followed by basketball and athletics.
Conclusion
LBP is frequent among undergraduate students of a sports and physical education institute in Tunisia. It is strongly associated with fatigue after the long periods of training in different sports. Gymnastics, judo, handball, and volleyball were identified as high-risk sports for causing LBP.
Regular physical activity of moderate intensity, such as walking, cycling, or other sports, has significant benefits for health. Moreover, regular and adequate levels of physical activity reduce the risk of falls as well as hip or vertebral fractures, and are fundamental to energy balance and weight control (Citation1). Unfortunately, these benefits are balanced by the risk of sports-related injuries (Citation2, Citation3).
Low back pain (LBP) is the most common orthopedic problem worldwide and is known to affect both younger and older adults (Citation4). The relationship between sports and LBP in adolescents appears to be curvilinear, and all levels of physical activity are associated with an increased risk of LBP in adolescents (Citation5, Citation6). The particularity of physical activity has also been related to risk of LBP in adolescents, and special risks are posed by activities that put a lot of stress on the lumbar spine (Citation7–Citation9), such as gymnastics, wrestling, rowing, diving, and football. Other sports such as swimming that put less pressure on the lumbar spine have a lower risk of causing LBP (Citation6).
Van Hilst et al. (Citation10) assessed the risk factors for and the prevalence of LBP among elite youth athletes in three sports: field hockey, speed skating, and football. They indicated that there is a strong connection between certain sports and LBP. The authors explained that certain motions, stresses, and actions of the athlete may influence LBP.
The literature review of Balagué et al. (Citation11) on the epidemiology of LBP in children and adolescents shows that the prevalence of LBP is higher among girls than among boys (Citation12–Citation17). Moreover, both prevalence and incidence of back pain increase with age (Citation12, Citation18–Citation21), in addition to possible roles for genetic (Citation22, Citation23) and psychosocial factors (Citation24, Citation25), school performance (Citation26, Citation27), and/or television watching (Citation14, Citation21) (Citation27). There are also associations between back pain and anthropometric parameters (Citation16, Citation28), smoking (Citation29), spinal mobility, and/or flexibility of muscles and joints (Citation16, Citation19).
LBP is estimated to occur in 10–15% of young athletes (Citation30), but the prevalence may be higher in certain sports (Citation6, Citation14) (Citation31–Citation33). In sports institutes, students spend a substantial amount of time in individual and team sports. These activities, such as physically heavy work, lifting, bending, twisting, pulling, pushing, and vibrations, have often been associated with LBP (Citation34).
This study aimed to determine the prevalence of LBP among students at a sports and physical education institute in Tunisia from 2006 until 2013.
Methods
Participants
This is a retrospective cross-sectional survey involving students at the Higher Institute of Sport and Physical Education in the city of Sfax. Students were both males and females aged 18.5–24.5 years. Data on age, weight, height, and smoking habits are collected routinely when students join the institute, and then the sport in which the student is injured in the low back is registered in the institute health service files. We collected information from the academic year of 2005–2006 until 2012–2013. Only students injured in the first or second year were taken into account, because the following years involve only athletics and gymnastics. Body mass index (BMI; kg/m2) was determined for each participant by dividing the weight in kilogram by the square of the height in meter. In this study we used the standard BMI with categories of underweight (BMI of <18.5), normal weight (BMI of 18.5−<25), overweight (BMI of 25−<30), and obesity (BMI of ≥30). Smoking was categorized as non-smoker, <20 cigarettes per day, and ≥20 cigarettes per day. BMI, smoking habits, and history of any pain or injuries were taken for all the students in the beginning of the first grade. Thus, we registered only students who were injured in the institute. Students with a previous history of LBP were not included. On the basis of the collected data, participants were dichotomized into those with or without LBP, while indicating the sports discipline in which they were injured or that they were injured after cumulative fatigue due to the large number of hours spent in practicing sports and physical activities. In 1 week, all students practice for a total of 16.5 h, spending 1.5 h in each of the following sports: soccer, handball, basketball, volleyball, judo, weightlifting, swimming, athletics, and gymnastics. In addition, athletics and gymnastics are practiced twice a week. LBP was defined as pain or discomfort in the low-back region, from the lower rib curvature to the lower part of the seat region. The question used systematically by the doctor of the institute health service to identify and estimate LBP cases was about the present injury and if and when they had LBP in the past. Thus, in cases of severe injuries the students are transported to the hospital. Furthermore, every registered injury causing LBP was recorded with its severity, but the most important detail for us was the sport in which the student was injured. Students who were injured more than one time were taken into account as subjects with LBP only for their first injury. The scientific council of the University of Sfax in Tunisia gave written permission for the study protocol.
Statistical analysis
Statistical analyses were done using the SPSS statistical package, version 11.5 (SPSS, Inc., Chicago, IL, USA). The chi-square test was used to test associations between LBP and other categorical variables (sex, obesity, and smoking habit), and to compare the prevalence of LBP between males and female. Statistical significance required that the p value be less than 0.05.
Results
Age and anthropometric data of the participants are presented in .
Table 1 Anthropometric characteristics of subjects with and without lower back pain
shows that the prevalence of LBP was significantly higher (p<0.001) among females (17.6%) than among males (12.5%). LBP prevalence did not differ by BMI or smoking habit (p>0.05). LBP occurred in 17.1% of those classified by BMI as lean, 14.8% of those in the normal range, 14.3% among those who were overweight, and 12.7% of those who were obese. In addition, 13.9% of students smoking <20 cigarettes and 13.3% of students smoking ≥20 cigarettes had LBP.
Table 2 Prevalence of lower back pain (LBP) by gender, obesity and smoking
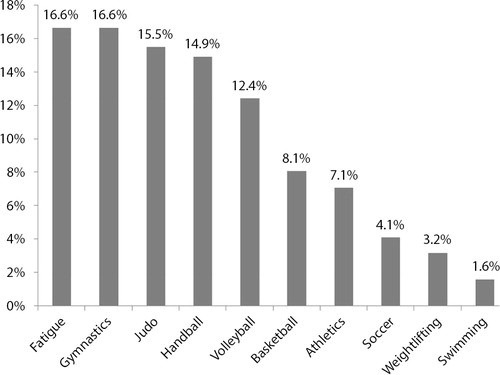
In the analysis of risk factors for LBP in sports training, we found that in both sexes combined, LBP was positively associated with fatigue (caused by the long time spent in training), gymnastics, judo, handball, and volleyball. The increased prevalence of LBP is less in basketball and athletics and even lower in soccer, weightlifting, and swimming ().
Fig. 1 Percent prevalence of lower back pain related to fatigue and type of sports in males and females combined.
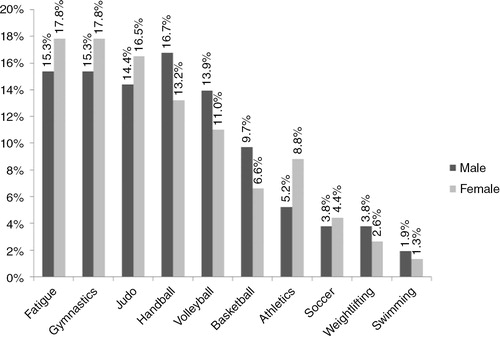
shows that there is no significant difference (p>0.05) in the prevalence of LBP among males and females separately if they are compared in each practiced sport at the institute. However, if we analyze the prevalence of LBP in terms of sex in each sport, we find that the prevalence of LBP was significantly higher among males than females in handball (p<0.05) and significantly lower in athletics (p<0.05).
Fig. 2 Percent prevalence of lower back pain related to fatigue and type of sports in males and females.
Discussion
Back pain is a highly prevalent health problem worldwide. Its incidence and prevalence are so high that it should be studied as an epidemic and social disorder (Citation35). The first salient feature that emerges from this study is that LBP is widespread among students in high schools for athletes (14.8%). The students were injured mainly in gymnastics, judo, handball, and volleyball, in addition to LBP caused by fatigue due to the long time spent in training.
These findings are generally in accordance with the literature. In a study focused on identifying the types of physical activity associated with increased occurrence of LBP in schoolchildren, Skoffer and Foldspang (Citation6) noted that LBP was increased by the number of hours jogging, playing handball, and doing gymnastics. In addition, Sato et al. (Citation33) found that the odds ratio for the risk of experiencing LBP was significantly higher in most sports items compared with the no-sports group. The most frequently implicated sports were volleyball, athletics, judo, gymnastics, golf, and rugby, where the odds ratio exceeded 2.
Gymnastics involves repetitive flexion, extension, and torsion. Kirialanis et al. reported that injuries among gymnasts are anatomically widely distributed (Citation36). As in our study, much research (Citation6, Citation33) (Citation37) noted that gymnastics was associated with an increased prevalence of LBP.
Judo is a grappling style martial art with emphasis on dynamic throws and submissions, which can lead to substantial injuries due to the high velocity of the maneuvers (Citation38). We registered a high prevalence of LBP in judo, as noted in the study of Sato et al. (Citation33). Handball, which also includes repeated sudden and often rather violent movements, has been shown to be associated with LBP in our population and in other studies (Citation6, Citation33).
A previous study (Citation11) reported associations between participation in volleyball and LBP. Likewise, we noted that many students had LBP after volleyball sessions. This LBP may be due to the repetitive plyometric movements in this sport.
We observed a high prevalence of LBP associated with the fatigue caused by the long time spent in physical activity (16.5 h per week). LBP occurrence depends on the amount and intensity of physical activity. However, this point of view is attractive in terms of prevention as physical activity is amenable to behavioral intervention, and physical training programs at school and leisure activities may be adjusted to aim at strengthening the back (Citation6). Moreover, both physical inactivity and intensive sports activity have been associated with LBP in some studies (Citation28, Citation32) (Citation39–Citation41). Our results show that a greater amount of physical activity increased the risk of LBP mainly in gymnastics, judo, handball, and volleyball. The time spent in athletics and basketball was associated with LBP to a lesser extent. Moreover, it appears that soccer, weightlifting, and swimming are correlated with relatively low prevalence of LBP. Skoffer and Foldspang (Citation6) reported that of several sports activities, only swimming was associated with a decreased prevalence of LBP. Swimming activates the muscles of the trunk, for example, the erector muscles of the spine, so swimming might be a means to prevent LBP. However, our results on soccer are at odds with those of Bejia et al. (Citation42), who reported that soccer was positively associated with chronic LBP in Tunisian schoolchildren and adolescents. Similarly, our findings on weightlifting contrast with those of Calhoon and Fry (Citation43), who reported that LBP was one of the most frequent injuries in this sport. The loads used in weightlifting may put the back at risk of injury. The relatively low prevalence of LBP in our study in soccer and weightlifting may be due to the system of this sports and physical education institute which is focused mainly on knowing how to teach these sports (gestural technique and pedagogy) and not on researching performance.
Our study shows that the percentage of females (17.6%) with LBP was significantly higher than that of males (12.5%), as frequently reported in the literature (Citation12–Citation17). However, the prevalence rates of LBP do not differ significantly between males and females (p>0.05) if they are compared in each practiced sport separately. There was no significant difference in LBP by BMI (p>0.05), in males and in females combined as reported in other studies (Citation44, Citation45).
Altarac et al. (Citation46) found that smoking was linked to training injury. In addition, many other studies have reported that active smoking is a risk factor for back pain (Citation47, Citation48). However, we did not find a significant relationship between smoking and LBP (p>0.05). A surprising finding in the study of Wirth et al. (Citation49) was that parental smoking seemed to increase the risk of spinal pain for both genders. The role of smoking in the development of spinal pain needs further investigation.
We believe that students should perform exercises to strengthen the muscles of the arms and back, and increase coordination of the upper extremities and the lumbar region with regular activities that have been proven to be effective for the prevention of LBP. Swimming or gymnastics are the nearest sports to reach this aim as they seem to reduce LBP significantly (Citation50).
This study was a survey based on data from the institute health service files of 8 years and therefore had some limitations. To closely evaluate the relationship between LBP and sports activities, more information on the students is needed, including basic information such as their physical activity outside the institute. In this study, the diagnostic of LBP was performed by the doctor of the institute health service and mostly without medical imaging, which could have shown the severity of LBP. Imaging is used to show the severity of the injury rather than the severity of the pain associated with it.
Conclusion
LBP was strongly associated with the amount of time reserved to practice the different sports planned in this sports and physical education institute. The sports identified as posing the greatest risk for LBP were gymnastics, judo, handball, and volleyball, followed by basketball and athletics. Moreover, the prevalence of LBP was significantly greater among females than males.
Acknowledgements
We thank the infirmary (mainly Dr. Imed Ajili) and the administration of the Sports and Physical Education Institute of Sfax (Tunisia) for their assistance. We are grateful to all those who took part in this study.
Conflict of interest and funding
The authors declare that they have no conflicts of interest concerning this research.
References
- World Health Organization. Move for health: benefits of physical activity. 2014. Available from: http://www.who.int/mediacentre/factsheets/fs385/en/ [cited 12 November 2014]..
- Bijur PE, Trumble A, Harel Y, Overpeck MD, Jones D, Scheidt PC. Sports and recreation injuries in US children and adolescents. Arch Pediatr Adolesc Med. 1995; 149: 1009–16.
- Conn JM, Annest JL, Gilchrist J. Sports and recreation related injury episodes in the US population, 1997–99. Inj Prev. 2003; 9: 117–23.
- Aggarwal N, Anand T, Kishore J, Ingle GK. Low back pain and associated risk factors among undergraduate students of a medical college in Delhi. Educ Health (Abingdon). 2013; 26: 103–8. [PubMed Abstract].
- Auvinen J, Tammelin T, Zitting P, Taimela S, Karppinen J. Associations of physical activity and inactivity with low back pain in adolescents. Scand J Med Sci Sports. 2008; 18: 188–94.
- Skoffer B, Foldspang A. Physical activity and low-back pain in schoolchildren. Eur Spine J. 2008; 17: 373–9.
- Iwamoto J, Abe H, Tsukimura Y, Wakano K. Relationship between radiographic abnormalities of lumbar spine and incidence of low back pain in high school and college football players: a prospective study. Am J Sports Med. 2004; 32: 781–6.
- Kolt GS, Kirkby RJ. Epidemiology of injury in elite and subelite female gymnasts: a comparison of retrospective and prospective findings. Br J Sports Med. 1999; 33: 312–18.
- Lundin O, Hellstrom M, Nilsson I, Sward L. Back pain and radiological changes in the thoraco-lumbar spine of athletes: a long-term follow-up. Scand J Med Sci Sports. 2001; 11: 103–9.
- Van Hilst J, Hilgersom NF, Kuilman MC, Kuijer PP, Frings-Dresen MH. Low back pain in young elite field hockey players, football players and speed skaters: prevalence and riskfactors. J Back Musculoskelet Rehabil. 2015; 28: 67–73.
- Balagué F, Troussier B, Salminen JJ. Non-specific low back pain in children and adolescents: risk factors. Eur Spine J. 1999; 8: 429–38.
- Salminen J, Pentti J, Terho P. Low back pain and disability in 14-year-old schoolchildren. Acta Paediatr. 1992; 81: 1035–9.
- Salminen JJ. The adolescent back. A field survey of 370 Finnish schoolchildren. Acta Paediatr Scand Suppl. 1984; 315: 1–122.
- Balagué F, Dutoit G, Waldburger M. Low back pain in schoolchildren. An epidemiological study. Scand J Rehabil Med. 1988; 20: 175–9.
- Brattberg G. The incidence of back pain and headache among Swedish school children. Qual Life Res. 1994; 3(Suppl 1): S27–31.
- Fairbank JCT, Pynsent PB, Van Poortvliet JA, Phillips H. Influences of anthropometric factors and joint laxity in the incidence of adolescent back pain. Spine. 1984; 9: 461–4.
- Viikari-Juntura E, Vuori J, Silverstein A, Kalimo R, Kuosma E, Videman T. A life-long prospective study on the role of psychosocial factors in neck–shoulder and low-back pain. Spine. 1991; 16: 1056–61.
- Burton AK, Clarke RD, McClune TD, Tillotson KM. The natural history of low back pain in adolescents. Spine. 1996; 21: 2323–8.
- Mierau D, Cassidy JD, Yong-Hing K. Low-back pain and straight leg raising in children and adolescents. Spine. 1989; 14: 526–8.
- Olsen TL, Anderson RL, Dearwater SR, Kriska AM, Cauley JA, Aaron DJ, etal. The epidemiology of low back pain in an adolescent population. Am J Public Health. 1992; 82: 606–8.
- Troussier B, Davoine B, de Gaudemaris R, Fauconnier J, Phelip X. Back pain in school children. A study among 1178 people. Scand J Rehabil Med. 1994; 26: 143–6. [PubMed Abstract].
- Matsui H, Terahata N, Tsuji H, Hirano N, Naruse Y. Familial predisposition and clustering for juvenile lumbar disc herniation. Spine. 1992; 17: 1323–8.
- Varlotta G, Brown M, Kelsey J, Golden AL. Familial predisposition for herniation of a lumbar disc in patients who are less than twenty-one years old. J Bone Joint Surg Am. 1991; 73: 124–8. [PubMed Abstract].
- Schofferman J, Anderson D, Hines R, Smith G, Keane G. Childhood psychological trauma and chronic refractory low-back pain. Clin J Pain. 1993; 9: 260–5.
- Schofferman J, Anderson D, Hines R, Smith G, White A. Childhood psychological trauma correlates with unsuccessful lumbar spine surgery. Spine. 1992; 17(Suppl 6): S138–44.
- Porter R, Drinkall J, Porter D, Thorp L. The vertebral canal: II. Health and academic status, a clinical study. Spine. 1987; 12: 907–11.
- Balagué F, Nordin M, Skovron ML, Dutoit G, Yee A, Waldburger M. Non-specific low-back pain among schoolchildren: a field survey with analysis of some associated factors. J Spinal Disord. 1994; 7: 374–9.
- Salminen JJ, Erkintalo M, Laine M, Pentti J. Low-back pain in the young. A prospective three year follow-up study of subjects with and without low-back pain. Spine. 1995; 20: 2101–7.
- Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between smoking and low back pain: a meta-analysis. Am J Med. 2010; 123: 87.e7–35.
- d'Hemecourt PA, Gerbino PG 2nd, Micheli LJ. Back injuries in the young athlete. Clin Sports Med. 2000; 19: 663–79.
- Swärd L, Hellstrom M, Jacobssen B, Pëterson L. Back pain and radiologic changes in the thoraco-lumbar spine of athletes. Spine. 1990; 15: 124–9.
- Kujala U, Taimela S, Oksanen A, Salminen JJ. Lumbar mobility and low back pain during adolescence. A longitudinal three-year follow-up study in athletes and controls. Am J Sports Med. 1997; 25: 363–8.
- Sato T, Ito T, Hirano T, Morita O, Kikuchi R, Endo N, etal. Low back pain in childhood and adolescence: assessment of sports activities. Eur Spine J. 2011; 20: 94–9.
- Bongers PM, De Winter CR, Kompier MAJ, Hildebrandt VH. Psychosocial factors at work and musculoskeletel disease. Scand J Work Environ Health. 1993; 19: 297–312.
- Schmidt CO, Kohlmann T. What do we know about the symptoms of back pain? Epidemiological results on prevalence, incidence, progression and risk factors. Z Orthop Ihre Grenzgeb. 2005; 143: 292–8.
- Kirialanis P, Malliou P, Beneka A, Giannakopoulos K. Occurrence of acute lower limb injuries in artistic gymnasts in relation to event and exercise phase. Br J Sports Med. 2003; 37: 137–9.
- Purcell L, Micheli L. Low back pain in young athletes. Sports Health. 2009; 1: 212–22.
- Shepard NP, Westrick RB, Owens BD, Johnson MR. Bony avulsion injury of the pectoralis major in a 19 year-old male judo athlete: a case report. Int J Sports Phys Ther. 2013; 8: 862–70. [PubMed Abstract] [PubMed CentralFull Text].
- Kujala UM, Salminen JJ, Taimela S, Oksanen A, Jaakkola L. Subject characteristics and low back pain in young athletes and nonathletes. Med Sci Sports Exerc. 1992; 24: 627–32.
- Kujala UM, Taimela S, Viljanen T. Leisure physical activity and various pain symptoms among adolescents. Br J Sports Med. 1999; 33: 325–8.
- Newcomer K, Sinaki M. Low back pain and its relationship to back strength and physical activity in children. Acta Paediatr. 1996; 85: 1433–9.
- Bejia I, Abid N, Ben Salem K, Letaief M, Younes M, Touzi M, etal. Low back pain in a cohort of 622 Tunisian schoolchildren and adolescents: an epidemiological study. Eur Spine J. 2005; 14: 331–6.
- Calhoon G, Fry AC. Injury rates and profiles of elite competitive weightlifters. J Athl Train. 1999; 34: 232–8. [PubMed Abstract] [PubMed CentralFull Text].
- Hou ZH, Shi JG, Ye H, Ni ZM, Yao J, Zheng LB, etal. Prevalence of low back pain among soldiers at an army base. Chin Med J (Engl). 2013; 126: 679–82. [PubMed Abstract].
- Tsuritani I, Honda R, Noborisaka Y, Ishida M, Ishizaki M, Yamada Y. Impact of obesity on musculoskeletal pain and difficulty of daily movements in Japanese middle-aged women. Maturitas. 2002; 42: 23–30.
- Altarac M, Gardner JW, Popovich RM, Potter R, Knapik JJ, Jones BH. Cigarette smoking and exercise-related injuries among young men and women. Am J Prev Med. 2000; 18(Suppl 3): 96–102.
- Cardon G, Balague F. Low back pain prevention's effects in schoolchildren. What is the evidence?. Eur Spine J. 2004; 13: 663–79.
- Roth-Isigkeit A, Schwarzenberger J, Baumeier W, Meier T, Lindig M, Schmucker P. Risk factors for back pain in children and adolescents. Schmerz. 2005; 19: 535–43.
- Wirth B, Knecht C, Humphreys K. Spine day 2012: spinal pain in Swiss school children–epidemiology and risk factors. BMC Pediatr. 2013; 13: 159.
- Harreby M, Hesselsøe G, Kjer J, Neergaard K. Low back pain and physical exercise in leisure time in 38-year-old men and women: a 25-year prospective cohort study of 640 school children. Eur Spine J. 1997; 6: 181–6.