

ABSTRACT
Introduction
Asthma is one of the most common chronic diseases worldwide. As a disease of the respiratory tract, the site of entry for the SARS-CoV-2 virus, there may be an important interplay between asthma and COVID-19 disease.
Areas covered
We report asthma prevalence among hospitalized cohorts with COVID-19. Those with non-allergic and severe asthma may be at increased risk of a worsened clinical outcome from COVID-19 infection. We explore the epidemiology of asthma as a risk factor for the severity of COVID-19 infection. We then consider the role COVID-19 may play in leading to exacerbations of asthma. The impact of asthma endotype on outcome is discussed. Lastly, we address the safety of common asthma therapeutics. A literature search was performed with relevant terms for each of the sections of the review using PubMed, Google Scholar, and Medline.
Expert opinion
Asthma diagnosis may be a risk factor for severe COVID-19 especially for those with severe disease or nonallergic phenotypes. COVID-19 does not appear to provoke asthma exacerbations and asthma therapeutics should be continued for patients with exposure to COVID-19. Clearly much regarding this topic remains unknown and we identify some key questions that may be of interest for future researchers.
Article Highlights
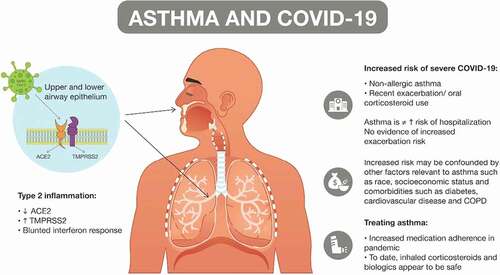
Increased risk of poor clinical outcomes with COVID-19 infection have been observed in those with more severe asthma and in those with nonallergic, or type 2 low asthma endotypes.
Presence of other high-risk comorbidities that are common in those with asthma may strongly influence outcome of COVID 19 infection.
COVID-19 infection has not been identified as a trigger of asthma exacerbation and reduced healthcare utilization for asthma during the pandemic is likely multifactorial.
Worsened outcomes related to COVID-19 infection in those with specific asthma endotypes may be related to aberrant interferon responses and variations in ACE 2 and TMPRSS2 expression associated with a type 2 airway inflammatory response.
Inhaled corticosteroids and asthma biologics should be continued through the course of illness to maintain asthma control.
Declaration of Interests
Dr. Rogers has the following relationships related to asthma research: Sanofi (asthma research funding, clinical investigator, and advisory board member), Astra Zeneca (clinical investigator, advisory board member, and funding for development of educational programs), Novartis (advisory board member).
The other authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.