

ABSTRACT
In this article, we update our earlier analyses of myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) economic impact and its National Institutes of Health (NIH) funding versus disease burden, taking into account the anticipated new cases of ME/CFS resulting from COVID-19. Prior to the COVID pandemic, we estimated a United States ME/CFS prevalence of 1.5 million and an annual economic impact of $36–51 billion. Now, due to COVID and its resulting post-acute sequalae, we estimate total ME/CFS prevalence could rise to between five and nine million. This would incur an annual U.S. economic impact of $149 to $362 billion in medical expenses and lost income, exclusive of other costs, such as disability benefits, social services, and lost wages of caretakers. NIH funding for ME/CFS research would need to expand from the current amount of $15 million per year to approximately $472–$600 million annually, up to a 40-fold increase, to be commensurate with that of similarly burdensome diseases.
Funding versus burden analysis
NIH funding for ME/CFS has been flat at $14–15 million annually since 2017, less than 262 other NIH-funded conditions and significantly less than diseases with comparable or less prevalence and/or disease burden [Citation43]. For comparison, in 2020, NIH issued $30.8 billion in extramural grants of which multiple sclerosis received $124 million, lupus $134 million, and HIV/AIDS $3.1 billion [Citation44]. In our 2020 analysis of funding versus disease burden, we showed that ME/CFS annual funding would need to be roughly $203 million to be commensurate with disease burden [Citation45]. That analysis used NIH’s 2015 burden data on 72 common diseases and the 2017 funding data for those diseases. Since that time, NIH has released burden data from 2017 [Citation46] and funding data from 2020 [Citation47]. In parallel, the ME/CFS pediatric prevalence estimate has been revised upwards, resulting in a larger pediatric component of the total prevalence [Citation14].
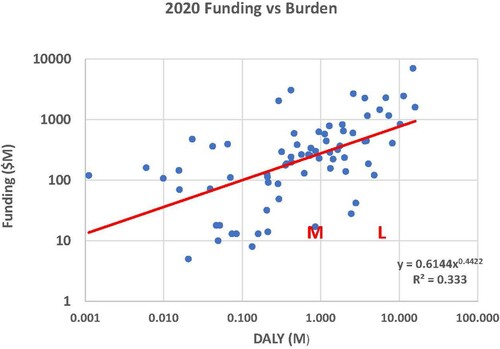
Using this updated data, we estimate ME/CFS disease burden and compare this to its NIH funding level. Disease burden for the 73 diseases in NIH’s analysis, represented in units of Disability Adjusted Life Year (DALY), is estimated for 2020 by extrapolating the 2017 values based on the increase in population from 2017 to 2020. This does not account for any changes in disability weights, prevalence rates, and mortality rates that may have occurred over this time period but are not yet reported. As the disease burden and funding data range over several orders of magnitude, we invoke a power law regression analysis. Results are presented in . The dots represent funding for the various diseases and conditions, with burden represented horizontally and funding vertically. Results are shown using a logarithmic scale. The solid line represents the optimal power-law fit to the data.
Figure 1. 2020 Funding ($M) versus 2020 Disease Burden (DALY, measured in millions, extrapolated from NIH’s 2017 values based on the increase in population from 2017 to 2020). (This DALY extrapolation does not account for any changes in disability weights, prevalence rates, and mortality rates over this time period and not yet reported.) The dots correspond to the diseases/conditions provided in the NIH analysis of funding versus burden. Results are shown using a logarithmic scale. The solid line represents the optimal power-law fit to the data, given by Funding = 0.6144*DALY^0.4422, where funding is measured in millions of dollars. The M corresponds to ME/CFS funding and burden prior to the COVID pandemic, and the L represents the expected ME/CFS burden due to onset following COVID.
The DALY for ME/CFS is calculated as the sum of the years lost due to disability (YLD) and years lost due to death (YLL). We previously postulated that for ME/CFS
where P is the total ME/CFS prevalence [Citation47]. Here, 0.46 is the ME/CFS disability weight, a factor that reflects the severity of a disease on a scale from 0 (perfect health) to 1 (equivalent to death). We also found that YLL = 0.226 million when the adult prevalence (PA) = 1.02M, giving
The factor 0.22 reflects the increased death due to cancer, heart disease, and suicide. Because the studies used to estimate loss due to death involved only adults and considering the very low pediatric death rate due to the aforementioned causes, we include only the adult prevalence in the calculation of YLL.
Based on earlier research, we estimate the adult prevalence to be 0.0042 times the adult population [Citation13], and the pediatric (ages 5–17) prevalence (PC) 0.0075 times the pediatric population in that age range [Citation14]. Estimates of ME/CFS prevalence vary significantly because of differences in case criteria and study conduct differences [Citation48]. We chose these estimates because they are supported by well-designed community-based studies with a clinical confirmation of diagnosis. Additionally, one must be careful not to use prevalence estimates where ME/CFS has been conflated with the symptom of chronic fatigue. This is problematic when relying on electronic health records in the United States, because the ICD-10-CM, implemented in 2015, uses the same ICD code for both ME/CFS and the symptom of unspecified chronic fatigue [Citation49].
With approximately 78% of the U.S. population consisting of adults and 16% children ages 5–17 [Citation50], we can express the adult and pediatric prevalence rates as
where N is the total U.S. population, which was 331.5 million in 2020 [Citation51]. This gives PA = 1.09 million and PC = 0.40 million, for a total prevalence of 1.49 million in 2020. This results in
for a 2020 ME/CFS DALY of 0.921 million. Plugging that value of DALY into the aforementioned power law regression analysis formula 0.6144*DALY^0.4422 (see ) yields a burden-commensurate funding level of $267 million. As in our earlier analyses, this estimate of DALY and of research funding commensurate with disease burden is based on the best available information about ME/CFS prevalence, level of disability, rates of premature death and resultant years of life lost. But the underlying information is scarce and not always aligned, which could affect the accuracy of these estimates as discussed in the study limitations. Nonetheless, at $267 million, the burden commensurate funding is nearly 18 times the NIH-reported funding level of $15 million for 2020 [Citation43]. Furthermore, the ME/CFS funding level normalized to that which is burden-commensurate is lower than that of any of the 73 diseases included in the latest NIH funding versus burden analysis.
The impact of COVID-19 on disease burden and burden-commensurate funding
We now examine the impact of ME/CFS onset following COVID-19 in the 2020–2022 timeframe on the 2020 pre-pandemic funding versus burden analysis. The NIH funding versus disease burden analysis is based on 2020 NIH funding, the latest year for which actual funding information is available, so we treat 2022 post-COVID cases of ME/CFS as if present in 2020.
According to the CDC, there have been approximately 76.8 million COVID cases in the U.S. and 0.9 million deaths as of 7 February 2022 [Citation52], hence 75.9 million COVID survivors. Of those, approximately 18.4% are children [Citation53], which equates to 61.9 million adult and 14.0 million pediatric COVID survivors. As discussed earlier, Komaroff and Bateman estimated 10% of COVID survivors would develop ME/CFS [Citation42]. To be conservative, we consider two scenarios – a 5% onset rate of post-COVID ME/CFS and a 10% onset rate. The former translates to 3.1 million adult and 0.7 million pediatric new cases of ME/CFS, and the latter to 6.2 million adult and 1.4 million pediatric new cases.
Adding these new post-COVID ME/CFS cases to the pre-pandemic (2020) adult and pediatric ME/CFS prevalences of 1.1 million and 0.4 million, respectively, results in a total of 4.2 million adult and 1.1 million pediatric cases for a 5% onset rate. For a 10% onset rate, the total prevalence is 7.3 million adults and 1.8 million children. The corresponding U.S. DALY values (calculated as above but using the revised prevalence rates) are 3.35 million for a 5% post-COVID ME/CFS onset rate and 5.77 million for a 10% onset rate. Plugging these values into our derived power law regression analysis formula suggests annual NIH funding in 2020 dollars would have to be $472 million for a 5% onset rate and $600 million for a 10% onset rate to be commensurate with disease burden.
If indeed 10% of all those who survive COVID-19 do experience ME/CFS onset, as suggested by Komaroff and Bateman, ME/CFS research would need to be funded over half a billion dollars annually for its funding level to be commensurate with disease burden. This would require a 40-fold increase in funding from the 2021 $15M level. As noted above, the estimates for post-COVID ME/CFS DALY and burden commensurate funding have limitations, but the magnitude of this difference with current funding bears consideration.
The NIH is investing $1.15 billion over four years to investigate the post-acute sequelae of SARS-CoV-2 infection (PASC) [Citation4] and has launched the RECOVER initiative as part of this [Citation26]. Given the shared symptoms, the reported percent of cases meeting ME/CFS criteria, and the possibility of an overlapping post-infectious pathology noted above, it might be reasonable to assume that the RECOVER research will directly benefit ME/CFS. But experts and advocates have expressed concern that the RECOVER initiative has not sufficiently incorporated into its plan the existing expertise and knowledge about ME/CFS disease pathology or the proper identification and tracking of emergent ME/CFS cases [Citation54–56]. For the RECOVER investment to benefit people with ME/CFS, including those who are anticipated to develop ME/CFS following COVID-19, these concerns will need to be addressed.
Economic and societal impact
The economic impact of ME/CFS was previously estimated to range from $36 billion to $51 billion annually in medical expenses (direct costs) and lost income (indirect costs) [Citation12]. This analysis, based on prevalence and economic cost data from 2020, assumed a per-person cost for medical expenses ranging from $3712 to $13750, and a per-person cost for lost income of $27,880 (averaged across those who can work and those who cannot). We extrapolate these cost estimates to 2022, resulting in an estimated increase in medical costs from 2020 to 2022 of 14% [Citation57], and an estimated increase in wages of 8.2% [Citation58]. This gives a per-person cost for medical expenses ranging from $4230 to $15,669, and a per-person cost of lost income of $30,200. Extrapolating from 2020 figures to account for population growth, there are 1.10 million adults and 0.40 million children with ME/CFS in 2022 (exclusive of new cases following COVID-19). This translates to an annual economic impact of $39 billion to $57 billion in 2022 dollars for non-COVID related ME/CFS. While the underlying studies applied to adults, we made the assumptions that pediatric and adult direct costs could be taken as the same, and that pediatric indirect costs would be small enough to ignore. We maintain those assumptions here.
We now estimate the direct and indirect costs for the combined cases of COVID-related ME/CFS and non-COVID-related ME/CFS. For a post-COVID ME/CFS onset rate of 5%, the combined prevalence of ME/CFS would be 4.2 million in adults and 1.1 million in children. This translates to direct costs ranging from $22 billion to $83 billion and indirect costs of $126 billion, for a total cost ranging from $149 billion to $209 billion in 2022 dollars. At a post-COVID ME/CFS onset rate of 10%, the combined prevalence would be 7.3 million in adults and 1.8 million in children. This translates to direct costs ranging from $38 billion to $142 billion, and indirect costs of $220 billion, for a total cost ranging from $258 billion to $362 billion in 2022 dollars.
Excluded from this analysis, but needing to be considered, are economic costs of disability services and social services associated with this highly disabled population, as well as lost income on the part of caretakers. Hence, including these costs, it would not be unexpected to see the total annual economic impact exceed a third of a trillion dollars.
Considering just cost is simplistic. Perhaps most important is the ongoing human suffering of people with ME/CFS because of a lack of treatments as a direct consequence of the lack of research funding. A significant increase in research funding is needed to reduce this tremendous economic, societal, and human impact.
Limitations
The computation of ME/CFS DALY in adults and children is significantly limited by the lack of robust studies of ME/CFS prevalence and the paucity of research into the natural history of ME/CFS, the magnitude, timing, and causes of premature deaths, and the level of disability experienced across the spectrum of disease severity. These were described in our 2016 [Citation47] and 2020 [Citation45] articles and apply here as well, as little new research has been done on these topics. The updated pediatric prevalence estimate is larger than previous estimates and has not been replicated yet but was used here because the study used more reliable methods than earlier studies, including more selective diagnostic criteria, a community-based recruitment approach that sampled 10,119 youth, and both a medical and psychological evaluation to identify ME/CFS in screened patients. While pediatric patients are clinically reported to have better prognosis than adults, we lack research on the level of physical and cognitive disability in children as a result of ME/CFS, so we assumed the disability weight to be the same as in adults, while the years lost due to pediatric death were assumed to be negligible.
In estimating the 2020 disease burden for ME/CFS, we extrapolated NIH’s 2017 DALY values to account for the increase in population from 2017 to 2020. This estimate assumes there were no changes in disability weights, prevalence rates, and mortality rates for the reported diseases over this time period.
Limitations on estimates of the economic impact of ME/CFS carry over from the 2020 paper [Citation12]. One is the estimate of $30,200 in lost income per person, which was extrapolated from Reynolds’ earlier estimate of annual lost income of $20,000 per person, averaged across those who could work and those who could not. This estimate assumed a greater percent of ME/CFS patients were able to work than what is reported today. This and other assumptions in Reynolds’ model could have underestimated the true value of lost income for ME/CFS. We also assumed that the average increase in medical expenses across diseases and the increase in wages for all workers would equally apply to people with ME/CFS. Finally, these cost estimates fail to account for the costs of disability services, needed social services, and lost income on the part of caretakers, which could be substantial.
Lack of research into Long COVID introduced a number of new limitations, starting with differences in the types of patients (e.g. hospitalized or not, positive COVID test or not, duration of illness) selected for a given Long COVID research cohort. While the research supporting the Komaroff and Bateman 10% estimate for the rate of development of post-infectious ME/CFS was based on adult cohorts and other infections, we inferred that 10% is a reasonable initial estimate for the development of ME/CFS following an acute SARS-CoV-2 infection in both adults and children. In computing the prevalence of post-COVID pediatric ME/CFS, it was not possible to break out the 5–17 age bracket used in the ME/CFS DALY estimate, but the additional cases of those younger than 5 are assumed to have an insignificant impact on the prevalence of post-COVID pediatric ME/CFS. We assumed that the rate of development of post-COVID ME/CFS along with the disability weight and death rate once ME/CFS develops does not change with sex, age, the severity of the initial disease, the COVID variant, the vaccination status, or as a result of the treatments used for COVID and Long COVID conditions over time. We also did not consider possible differences in the disability weight, death rate, cure rate, and duration of illness of post-COVID ME/CFS as compared to pre-COVID ME/CFS. Finally, we used the national estimate of 76.8 million cases of COVID and 0.9 million deaths, but that number is increasing and could also have been affected by lack of testing and reporting. All of the above assumptions are subject to change with further research.
In extending the funding versus burden analysis to account for post-COVID ME/CFS, we were faced with the conundrum of combining a 2022 post-COVID ME/CFS incidence with a 2020 analysis that reflected the pre-pandemic NIH funding and ME/CFS prevalence. Because 2022 NIH actual funding is not available, we chose to add the estimated 2022 post-COVID ME/CFS cases to the 2020 ME/CFS cases, treating them for the sake of this analysis as though they existed and met criteria in 2020.
We recognize that COVID could impact the prevalence and burden of other diseases as well. We did not consider those impacts and how that would affect the funding versus burden analysis.
Conclusions
A significant portion of people with Long COVID are likely to develop ME/CFS, contributing to a substantial increase in ME/CFS prevalence, disease burden, and economic impact. Taking into account this expected increase in ME/CFS onset following COVID-19, we estimate the resultant U.S. ME/CFS prevalence could range between 5 and 9 million individuals. This would require an annual research funding level of $472 to $600 million to be commensurate with its disease burden – up to 40 times higher than the current $15 million allocation. This increase in prevalence translates to an annual economic burden of ME/CFS of $149 to $362 billion in medical expenses and lost income, an amount that does not account for the economic costs associated with disability services and social services as well as lost income on the part of caretakers.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Arthur A. Mirin
Arthur A. Mirin is an Applied Mathematician and Independent Researcher from Castro Valley, CA.
Mary E. Dimmock
Mary E. Dimmock is an Advocate and Independent Researcher from Waterford, CT.
Leonard A. Jason
Leonard A. Jason is a Professor of Psychology and Director of the Center for Community Research at DePaul University.