
Figures & data
Figure 1 The clinical presentation of patients.
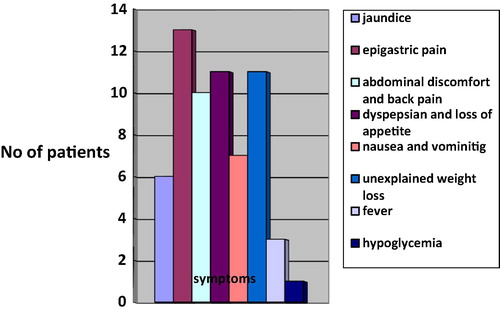
Table 1 MDCT diagnosis in relation to the number of patients.
Table 2 The age range distribution in the 30 included patients.
Table 3 CT severity index (CTSI) for grading of acute pancreatitis by Balthazar et al.
Figure 2 Irresectable pancreatic body adenocarcinoma T4N1 M1. Axial post contrast CT images (porto-venous phase) show pancreatic body hypodense mass lesion inducing focal contour bulge (white arrow) with loss of fat plane between it and the posterior wall of the stomach (thick arrow). There is also right hepatic lobe hypodense metastatic focal lesion (thin curved black arrow) and peri pancreatic nodal involvement (thin curved white arrow). The distal pancreatic duct is seen dilated (thick curved white arrow).

Figure 3 Irresectable pancreatic body carcinoma (T4 N0M1). Axial CT image shows hypodense heterogenous pancreatic body mass (white arrow) encasing the celiac trunk (black arrow) and atrophy of the pancreatic tail (arrowhead). Liver with multiple hypodense lesions due to metastasis (thick black arrow).
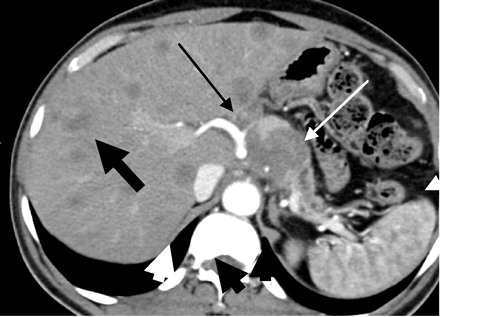
Table 4 TNM Classification for the staging of pancreatic cancer.Citation25
Table 5 CT severity index in case of acute pancreatitis.
Figure 4 Acute necrotizing pancreatitis CT SI 9. Note a fluid attenuation collection in the pancreatic bed with minute islands of preserved fatty tissue (thin arrow) and well defined rim, suggestive of walled off necrosis with fat necrosis involving the pancreas and peri pancreatic tissue. Few small areas of glandular enhancement are only seen at the region of the body and tail (thick arrow).
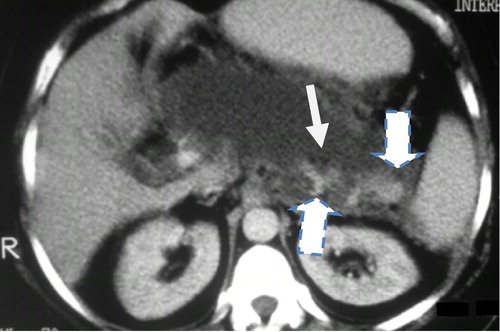
Figure 5 (a and b) Acute necrotizing pancreatitis with pancreatic necrosis and abscess formation. CTSI 10 Axial and coronal MDCT images showed Fluid attenuation collection at the pancreatic body, tail and part of the head with well-defined wall. It shows small fat density (thin arrow) and air (thick arrow) loculi, suggestive of infected pancreatic walled off necrosis and abscess formation. Percutaneous catheter is seen inside the collection for drainage.
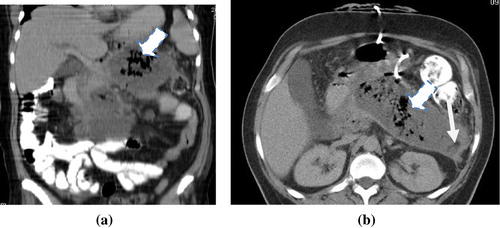
Figure 6 Axial MDCT image showed Enlarged/swollen pancreas with patchy ill-defined non enhancing areas of necrosis (thin arrows) are seen at the pancreatic head, body and tail. There is also stranding of the peri pancreatic fat and peri splenic fluid collection (thick arrow).
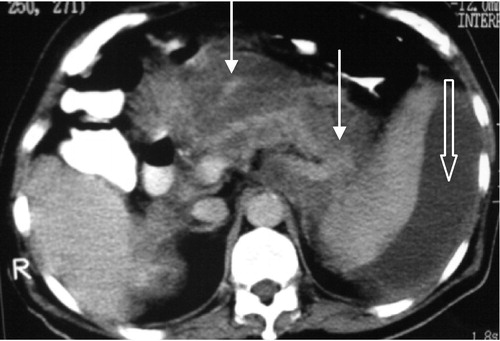
Figure 7 Chronic calcific pancreatitis with intra ductal stone and pseudopancreatic cyst. Axial CT images demonstrate atrophic pancreas with innumerable diffuse calcification. A well-defined homogenous fully encapsulated collection, representing pseudopancreatic cyst is seen related to the pancreatic head region (curved arrow).
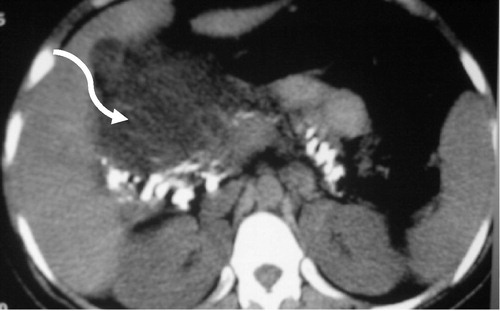
Table 6 Distribution of neoplastic pancreatic lesions according to pathological findings.
Table 7 The MDCT findings in pancreatic adenocarcinoma.
Figure 8 (a and b) Irresectable pancreatic head adenocarcinoma T4 N0M1. (a) Axial post contrast CT images (porto-venous phase) pancreatic head heterogeneously enhancing irregular mass lesion inducing contour bulge (white arrow) invading the CBD with consequent intra hepatic biliary dilatation (thin curved white arrow). There is also right hepatic lobe hypodense metastatic focal lesion (thin curved black arrow). (b) Coronal MIP reconstruction clearly shows the vascular invasion of the portal vein.
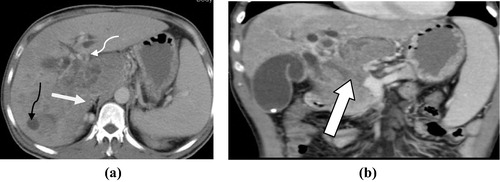
Figure 9 Benign pancreatic head insulinoma. Axial CT cut pancreatic-phase shows a 1 cm small, typically hyperenhancing nodule in the pancreatic head (arrow).

Table 8 Classification of patients according to resectability.