
Figures & data
Figure 1. Flow diagram of the systematic review process, including searches of databases and other sources.
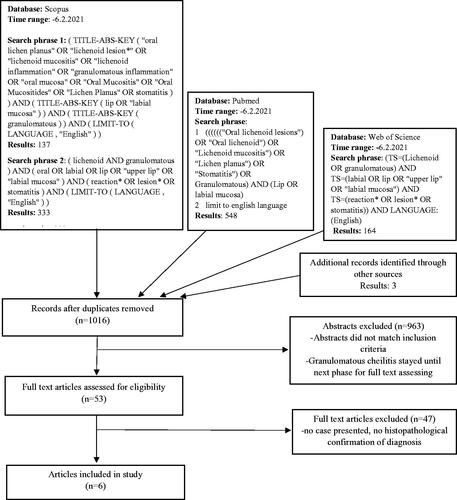
Figure 2. Histopathological findings from labial mucosal biopsies. (A, B) Hyperparakeratotic stratified squamous epithelium with saw-toothed rete ridges in some areas, basal cell degeneration, apoptotic basal keratinocytes (arrow in B) and inflammatory cell exocytosis. A dense band-like lymphocytic infiltration in the lamina propria and patchy inflammatory cell infiltrates in the submucosa. (C) An aggregate of monocytic inflammatory cells consisting mainly of lymphocytes, visible also perineurally (marked by the arrow). (D) Possible histiocytes visible in the infiltrate (indicated by the arrow). Haematoxylin and eosin stain, original magnification × 25 (A), × 200 (B), × 400 (C), × 400 (D).
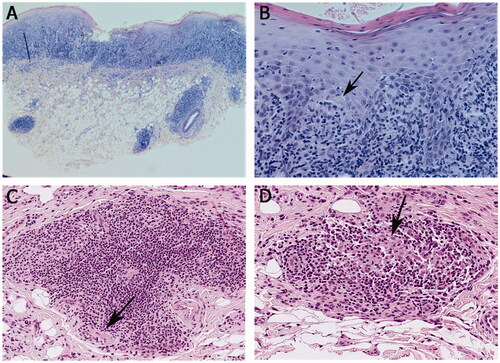
Figure 3. Clinical presentation of the upper labial mucosa and upper anterior labial gingiva over a 10-year span (A, B, D, and E). White reticular striae or papular lesions with erythema were seen at most visits. (C) A faint white stria to the labial mucosa after treatment with intralesional methylprednisolone (40 mg/ml) injection. (F) Slight erythema of the labial mucosa and gingiva on the last follow-up visit. The patient used tacrolimus when needed.
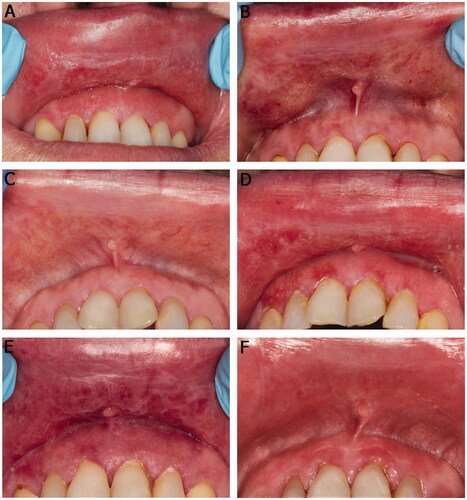
Table 1. Details of the demographic and clinical characteristics of the patients.
Table 2. Histopathological features of the lesions.