Figures & data
Table 1. Clinical characteristics and course of treatment of esophageal perforation in four cases.
Figure 1. (a–c) Endoscopic view of the esophageal defect in case II. Immediately after pneumatic dilatation, a laceration 3 cm above the Z-line was observed (a). The patient was treated with Eso-SPONGE® vacuum therapy (b). After 5 days, endoscopic inspection showed healing of the esophageal wall defect with granulation tissue (c).

Figure 2. (a–c) Endoscopic images of esophageal perforation in case III. The defect was located just above the esophagogastric junction (a) and was successfully closed with 15 endoclips (b and c).
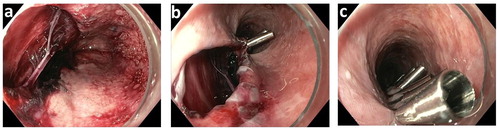
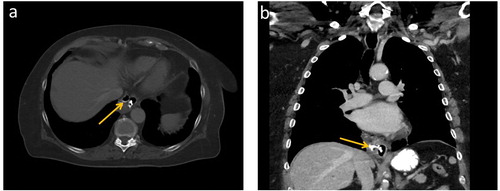
Figure 3. Axial (a) and coronal (b) CT scan of the chest showing evidence of contained esophageal perforation on the right side of the distal esophagus in case IV, including extraluminal air and contrast (arrows).