Figures & data
Figure 1. Landmarks in the anal canal seen under water: anorectal line, dentate line and the area between, the anal transitional zone. Purple arrowheads show a flat, slightly raised ASIL (anal squamous intraepithelial lesions) with widened and irregular IPCL (intra papillary capillary loops). Black arrowheads show an exophytic villous ASIL and the red arrowheads show an exophytic non-villous ASIL.
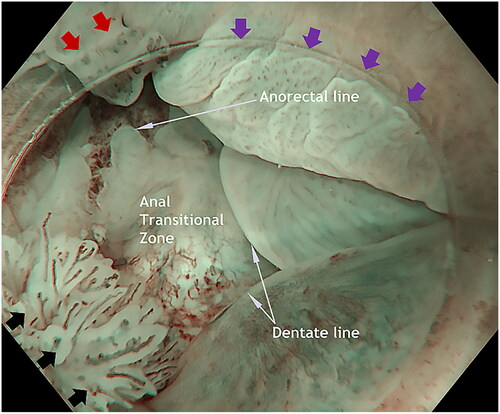
Figure 2. Creating a submucosal cushion under the lesion and also providing local anesthesia. Proximal and on the left side of the lesion is the mucosa paler after the previous injection. At 11 o’clock is an exophytic whitish non-villous exophytic ASIL.
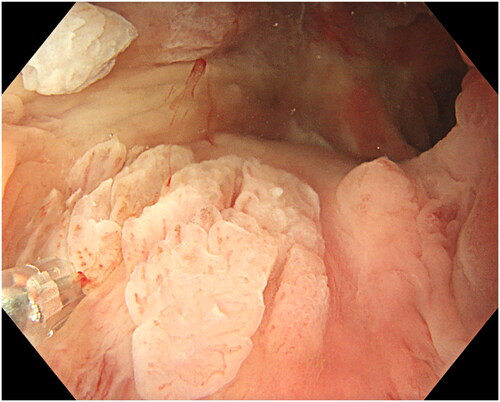
Figure 3. Placing the snare with a slight pressure. At the tip of the casing is a small non-villous exophytic ASIL.
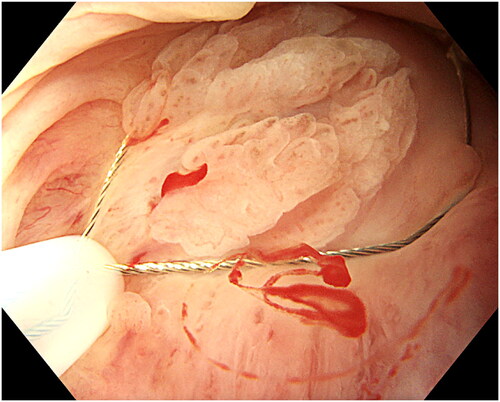
Figure 4. Resection of the lesion. The lesion is retrieved and sent for histopathology. Minor bleeding can be coagulated with the top of the snare. In case of uncertainty about radical resection, the edges can also be coagulated.
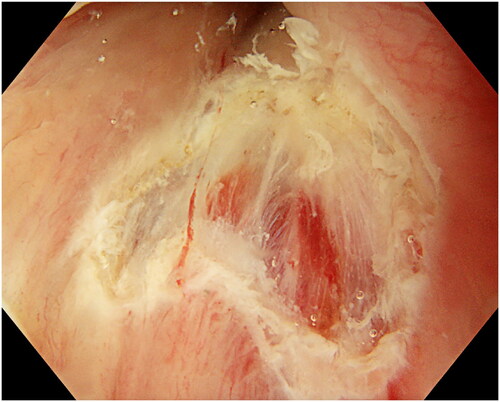
Table 1. Comparison between endoscopic and surgical treatment.
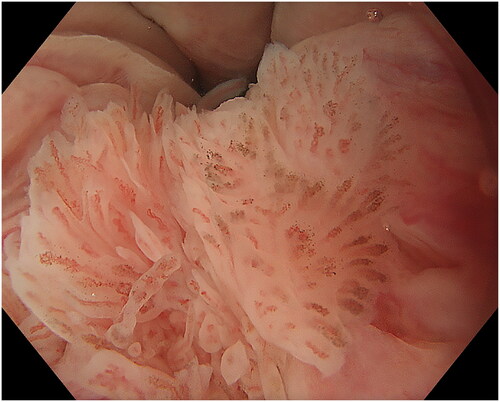
Figure 5. ASIL with a villous exophytic appearance with branchlike blood vessels.
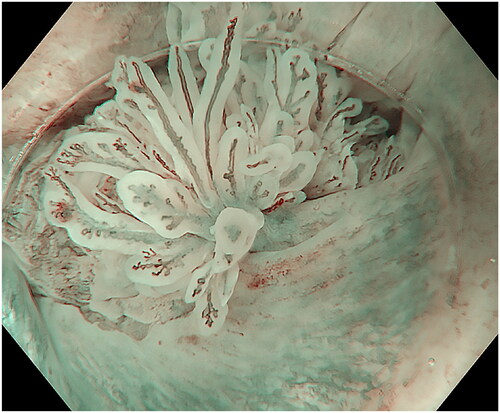
Figure 6. ASIL with a non-villous exophytic appearance.

Figure 7. ASIL with a nodular-granular configuration.

Figure 8. Slightly raised ASIL with changed intrapapillary capillary loops.
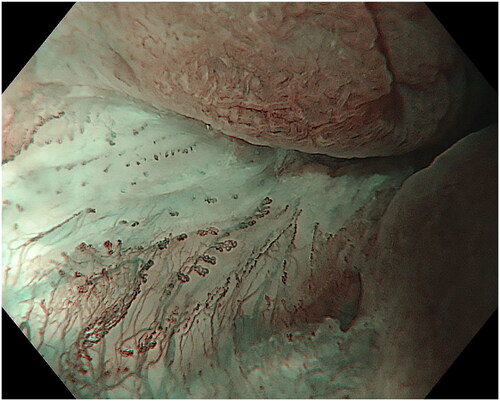
Figure 9. Non-raised ASIL with irregular and widened IPCL.
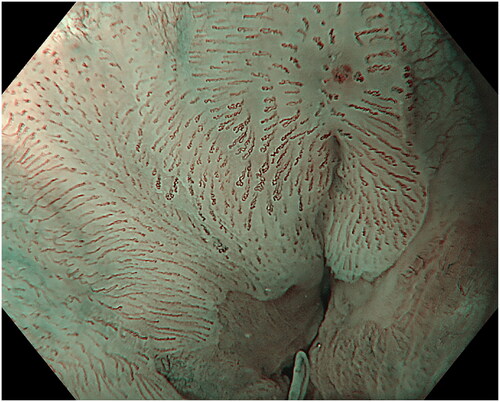
Figure 10. ASIL with brownish epithelium and brownish dots.