Figures & data
Table 1. Summary of immunohistochemical methodology.
Table 2. Summary of clinical signs, pathological findings and causes of death for the 8 meerkats in captivity.
Figure 1. Case 6. The dorsum and tail exhibit locally extensive area of chronic dermatitis with alopecia, crusting, hyperkeratosis and multifocal erosions and ulcers. Bar = 1 cm.
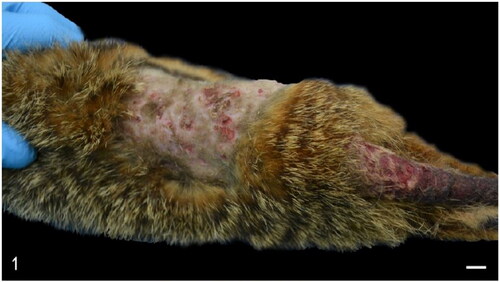
Figure 2. Case 1. Focally extensive peritoneal hemorrhage (arrows) as a result of a foreign body-induced duodenal perforation. Bar = 1 cm.
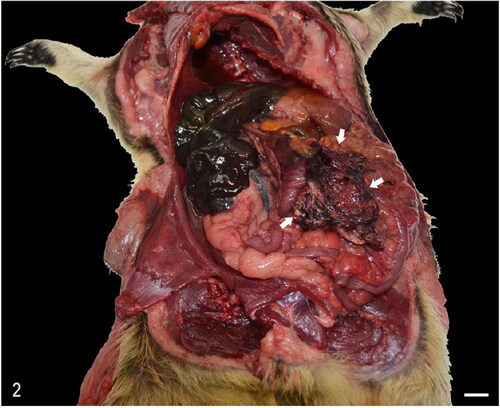
Figure 3. Case 3. The short gastric arteries are expanded by multifocal pale-yellow (atheromatous) plaques (arrows).
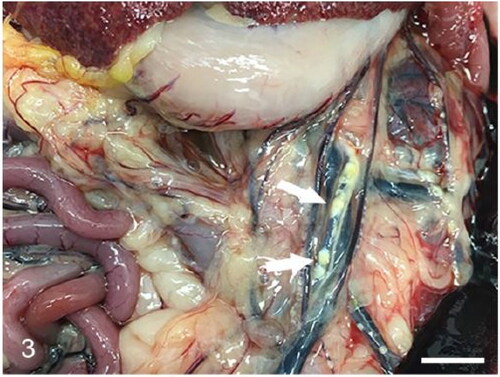
Figure 4. Case 3. The heart exhibits tortuous, yellow, stripes (arrows) that correspond with atheromatous branches of the coronary arteries, and pale areas of myocardium that correspond with areas of degeneration (asterisks).
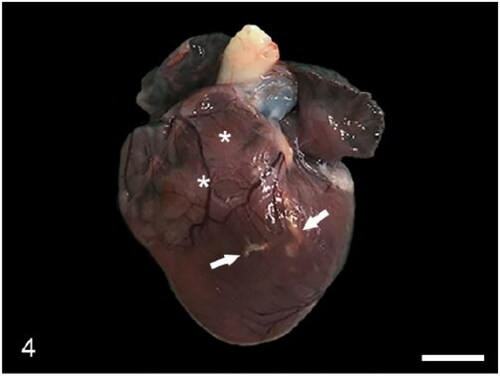
Figure 5. Case 3. The tunica media of a coronary artery is expanded by a mineralized atheromatous plaque (asterisk). The atheromatous plaque compresses a segment of the bundle of His (arrows). Bar = 50 µm.
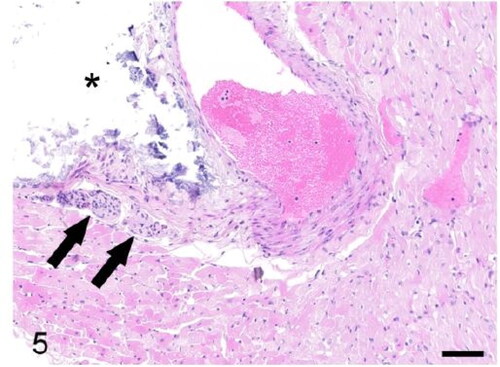
Figure 6. Case 3. Glomerulosclerosis. Glomerular capillaries are markedly thickened and degenerated. The Bowman’s capsule is also markedly thickened (asterisk). Bar = 20 µm.
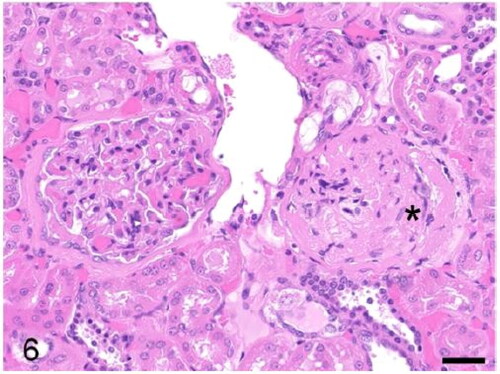
Figure 7. Case 2. The myocardium is infiltrated by lymphocytes, plasma cells and neutrophils (arrows). Bar = 20 µm.
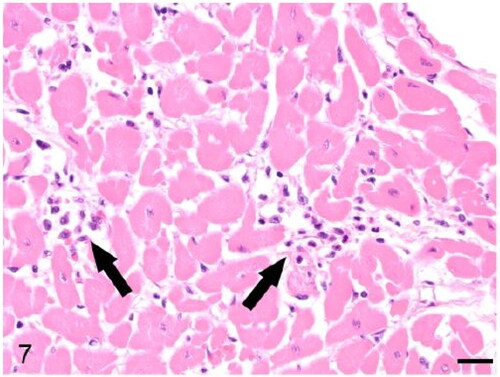
Figure 8. Case 3. Cholesterol granulomas expand the choroid plexus and compress the lateral ventricles and surrounding parenchyma. The third ventricle is dilated. Bar = 3 mm.
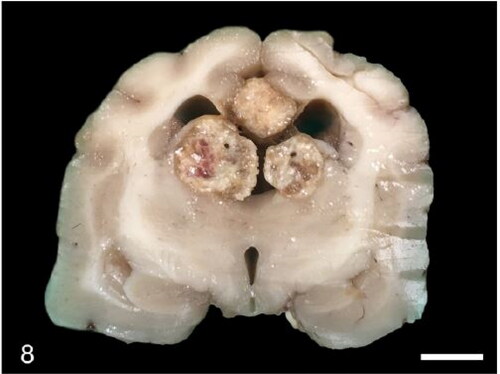
Figure 9. Case 3. A multinodular cholesterol granuloma compresses the lateral ventricles. The third ventricle is markedly dilated (asterisk). Inset: There is, hypercellularity, rarefaction and vacuolation of the neuropil (degeneration) and rare hemosiderin-laden macrophages (chronic haemorrhage). Bar = 3 mm.
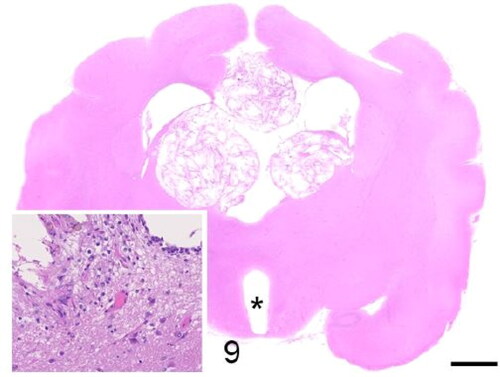
Figure 10. Case 8. Focal pulmonary cholesterol granuloma. Bars = 1 cm.

Figure 11. Case 2. Granulomatous pneumonia. The right caudal lung lobe is diffusely dark red, firm and enlarged (arrows). Bar = 1 cm.
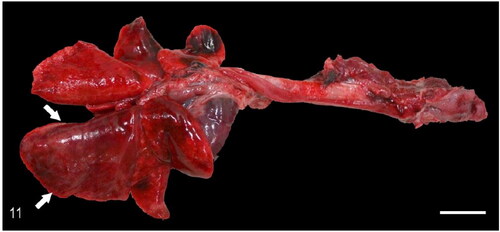
Figure 12. Case 3. Pulmonary adenomas. The right lung exhibits multifocal, white, firm, round nodules that rise the pleura. Bar = 1 cm.
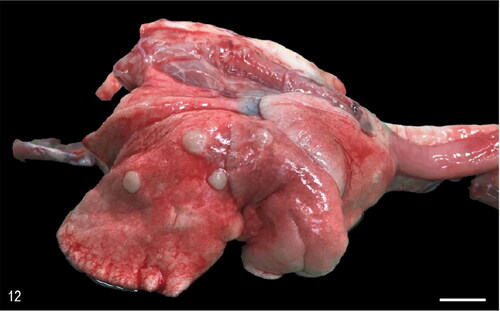
Figure 13. Case 2. Granulomatous pneumonia. The lung is locally extensively expanded by a pyogranulomatous inflammatory exudate (consolidation). Inset: A nematode larvae is surrounded by macrophages, eosinophils, lymphocytes, and plasma cells. There is marked pneumocyte type II hypertrophy. Bar = 1 mm.
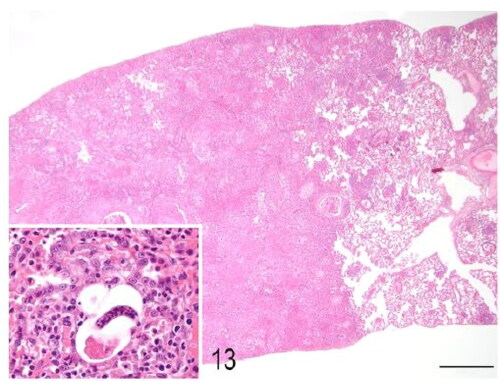
Figure 14. Case 3. Pulmonary adenomas. The lung parenchyma is expanded by variably sized well-demarcated epithelial neoplasms that compress the surrounding alveolar spaces. Inset: The neoplasms consist of clear cuboidal cells with defined margins and a single polarized nucleus. Cellular atypia is minimal. Bar = 1 mm.
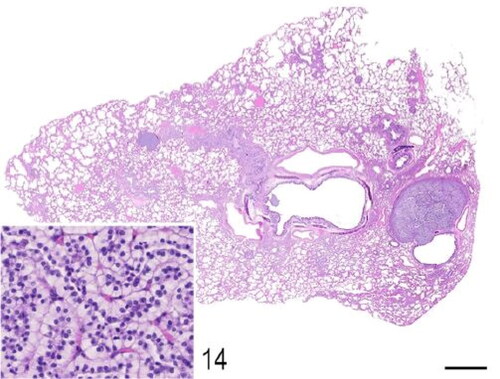
Figure 15. Case 3. The pulmonary adenoma was diffusely positive for multicytokeratin immunohistochemistry. Bar = 50 µm.
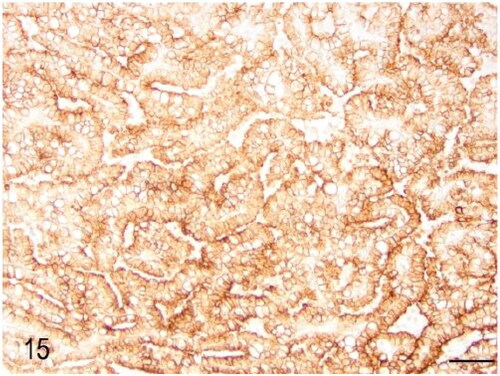
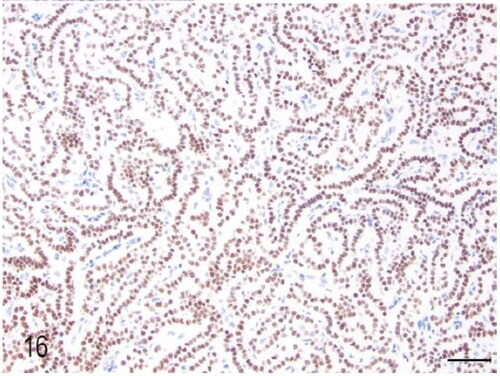
Figure 16. Case 3. The pulmonary adenoma was diffusely positive for TTF-1 immunohistochemistry. Bar = 50 µm.