Figures & data
Figure 1. Serial change of CT image following microwave ablation at high power. CT images taken before ablation (a,c) and within 10 min after ablation (b,d) for short (a,b) and long (c,d) duration energy delivery. Compared with CT before ablation (a, c), low density area appeared around the electrode, surrounded by ill-demarcated consolidation on CT immediately after both short (b) and long duration (d) energy delivery. Ablation after long duration (d) treatment appears more spherical when compared to short duration (b) of energy delivery. Dotted lines demarcate the ablation zone from untreated lung.
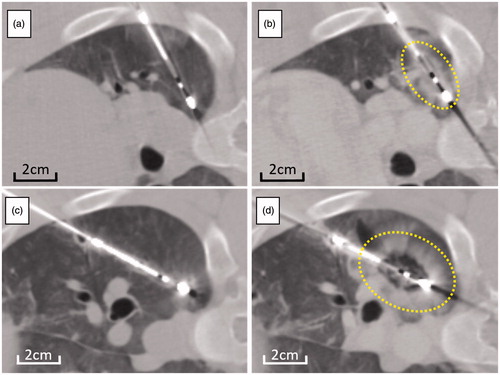
Table 1. Adverse event results.
Figure 2. Complications. (a) Pneumothorax; Pneumothorax appeared immediately after the removal of the antenna (*). This lesion was ablated with short duration of energy delivery. Air-filled needle tract connecting to pleural space (yellow arrow) was also visible. (b) Cavitation within the ablation; cavitation (blue arrow) was seen on CT at 7 d after the treatment and was completely enclosed with the ablation. This lesion was ablated with long duration of energy delivery. Dotted lines demarcate the ablation zone from untreated lung.
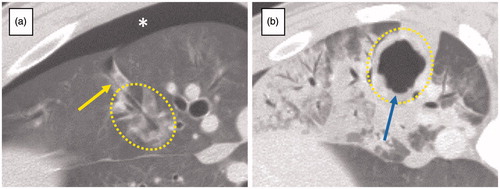
Table 2. CT Findings at day 0.
Figure 3. Histology of ablation zone. Histological specimen at day 2 (a, 1.25×, short duration) shows a well demarcated area of complete coagulation necrosis with a rim of hyperaemia, haemorrhage, and fibrin exudation at the edge of the area of necrosis. At day 28, a rim of dense fibrosis and inflammation characterised by infiltration by numerous neutrophils, macrophages, lymphocytes, and plasma cells is seen (b, 1.25×, long duration). Some lesions show cavitation within the dense rim (c, 1.25×, short duration). All bronchi were completely ablated inside the ablation zone. At day 2, the structure, including epithelium (blue arrow) or cartilage (yellow arrow) of bronchus is maintained (d, 20×, short-duration energy delivery), but is destroyed at day 28 (e, 20×, short-duration energy delivery). A 5mm pulmonary artery at the edge of the necrotic zone shows incomplete necrosis, and the ablation zone margin is concaved (f, 1.25×, short-duration energy delivery). A: ablated area; M: ablation margin; N: non-ablated area; *: antenna tract; V: pulmonary vein. Dotted lines demarcate the ablation zone from untreated lung.
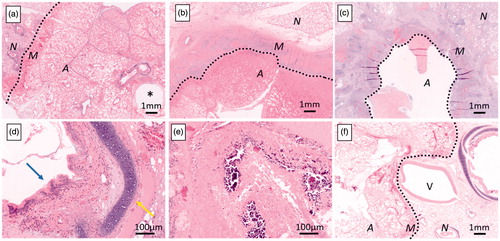
Table 3. Histological findings at days 2 and 28.
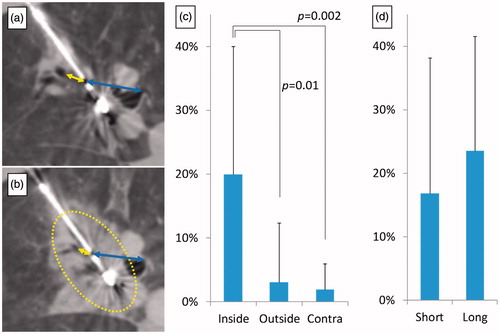
Figure 4. Distortion of lung tissue following high power microwave ablation. Distances between the centre of the ablation zone, and bronchus or large vessels both inside (yellow arrow) and outside (blue arrow) the ablation zone were measured on CT images before (a) and immediately after ablation (b). The distance between the ablation centre and these structures decreased significantly within the ablation when compared with structures outside the ablation zone, or equivalent measurements performed in untreated contralateral lung (c). The distortion ratio between short (2 min) and long duration (10 min) was not significantly different (d). Dotted lines demarcate the ablation zone from untreated lung.