
Figures & data
Figure 1. Patients’ selection.
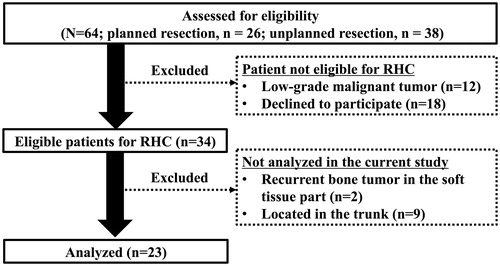
Figure 2. Radio-hyperthermo-chemotherapy protocol. Hyperthermia: Hyperthermia is performed using an 8-MHz radiofrequency capacity heating system (Thermotron RF-8; Yamamoto Vinita, Osaka, Japan) and repeated every week for a total of five courses. The objective of the hyperthermia was to achieve a temperature of 42.5 °C or more for 60 min. Chemotherapy: Chemotherapy is administered by intra-arterial (IA) infusion. During hyperthermia, cisplatin (first, third, and fifth sessions) or pirarubicin (an Adriamycin derivative; second and fourth sessions) are simultaneously injected. After five courses of IA chemotherapy, systemic chemotherapy using ifosfamide, pirarubicin, and etoposide are initiated, followed by surgery. Radiation: All patients are treated with daily radiotherapy at a dose of 40.0 Gy, for a total of 20 sessions. Irradiation is performed just before hyperthermia and chemotherapy on the day of hyperthermia and chemotherapy. The details of each course of RHC are described in Supplemental Figures 1 and 2.
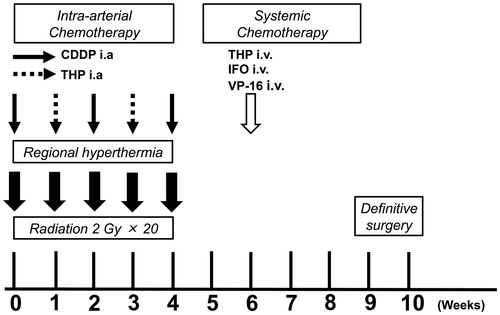
Figure 3. Schema of second-look surgery. *Transverse skin excision sometimes occurs like this schema. This procedure expands tumor contamination and requires extensive resection of muscles and skin.
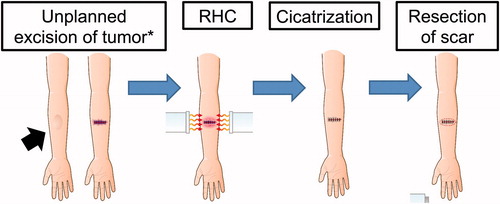
Figure 4. The representative case. A 64-year-old male patient was initially diagnosed with solitary fibrous tumor in the vastus femoris ([a] MRI T1WI, with gadolinium enhancement) and underwent wide resection 1 year ago. During the follow-up period, the recurrence of tumor was found around the femoral artery ([b], MRI T1WI, with gadolinium enhancement). Then, the RHC was performed for the recurrent tumor. The area of irradiation was determined by the radiologist with coverage of the prior surgical area. IA chemotherapy was administered from the catheter placed in the superficial femoral artery (c). The evaluation of thermal effect was mild (42.5 °C achieved in 3/5 RHC cycles). An example of thermal therapy is depicted in (d). Although the tumor size remained the same, the intake of tracer was attenuated (e). Then, a repeat wide resection was performed. Five years after surgery, the patient was still alive with no evidence of the disease.
![Figure 4. The representative case. A 64-year-old male patient was initially diagnosed with solitary fibrous tumor in the vastus femoris ([a] MRI T1WI, with gadolinium enhancement) and underwent wide resection 1 year ago. During the follow-up period, the recurrence of tumor was found around the femoral artery ([b], MRI T1WI, with gadolinium enhancement). Then, the RHC was performed for the recurrent tumor. The area of irradiation was determined by the radiologist with coverage of the prior surgical area. IA chemotherapy was administered from the catheter placed in the superficial femoral artery (c). The evaluation of thermal effect was mild (42.5 °C achieved in 3/5 RHC cycles). An example of thermal therapy is depicted in (d). Although the tumor size remained the same, the intake of tracer was attenuated (e). Then, a repeat wide resection was performed. Five years after surgery, the patient was still alive with no evidence of the disease.](/cms/asset/d8561c01-b5b0-449d-9065-e48c9540e0e6/ihyt_a_1518545_f0004_c.jpg)
Table 1. Clinicopathologic characteristics of patients with malignant soft tissue sarcomas undergoing radio-hyperthermo-chemotherapy (n = 23).
Figure 5. Oncologic outcomes of patients with highly malignant soft tissue sarcomas treated by radio-hyperthermo-chemotherapy (RHC). (a) Overall survival, (b) distant relapse-free survival, and (c) local control. The straight lines indicate the patients’ group who underwent RHC for salvage after unplanned resection and the dotted lines indicate the patients’ group who underwent RHC for recurrent lesion after planned resection. RHC: radio-hyperthermo-chemotherapy; OS: overall survival; D-RFS: distant relapse-free survival; LC: local control.
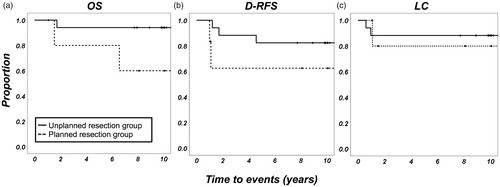
Table 2. Oncologic outcomes of the different histologic tumor types after undergoing radio-hyperthermo-chemotherapy (n = 23).
Table 3. Oncologic outcomes of patients undergoing radio-hyperthermo-chemotherapy (n = 23).
Supplemental Material
Download MS Power Point (61.1 KB)Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author SY on reasonable request.