
Figures & data
Table 1. Baseline characteristics of SHPT patients ineligible for surgical resection at the time of MWA (n = 35).
Figure 1. A 47-years-old female patient with a recurrent and ectopic SHPT nodule 2 years after parathyroidectomy was treated by microwave ablation (MWA). (A) A hypoechoic SHPT nodule (long thin arrow) closing to the right sympathetic nerve (short thin arrow) was disclosed to locate between the right carotid artery (long thick arrow) and jugular vein (short thick arrow) in ultrasound. (B) The CT scan showed that the SHPT nodule (long thin arrow) is between the right carotid artery (long thick arrow) and jugular vein (short thick arrow). (C) The SHPT nodule has radioactivity concentration (black arrow) in the late phase on MIBI scan. (D) A uniform hyperenhancement of the SHPT nodule (long thin arrow) between the right carotid artery (long thick arrow) and jugular vein (short thick arrow) was displayed in CEUS preablation. (E) The spacer fluid (white triangle) was injected around the right sympathetic nerve (short thin arrow) behind the right carotid artery (long thick arrow), jugular vein (short thick arrow) and SHPT nodule (long thin arrow) for preventing the nerve from thermal injury during ablation. (F) The hyperechoic signal emerging along the tip of antenna (white triangle) inside the SHPT nodule (long thin arrow) during ablation. (G) A non-enhancement area covered the SHPT nodule (long thin arrow) beside the jugular vein (short thick arrow) after MWA, suggesting complete ablation was achieved by MWA. (H) The SHPT nodule (long thin arrow) in front of right carotid artery (long thick arrow), jugular vein (short thick arrow) and sympathetic nerve (short thin arrow) was obviously shrinking 6 months after MWA in ultrasound.
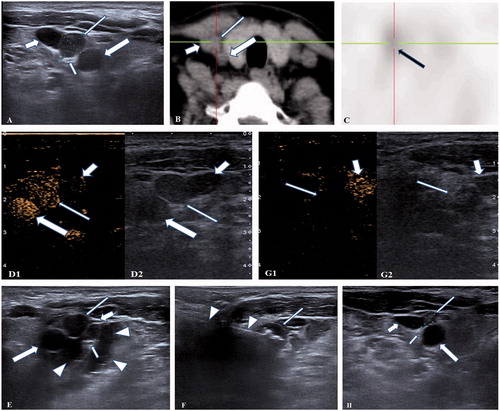
Table 2. Laboratory data of SHPT patients before and after MWA.