
Figures & data
Figure 1. Ablation therapies for lymph node metastases originating from hepatocellular carcinoma. (A) The preoperative MR imaging showed a porta hepatic LN metastasis. (B) The microwave antenna was advanced into the target lesion. (C) The MR imaging at 5 days later showed partial response and mild heterogenous enhancement. (D) The preoperative computed tomography scan showed a superior vena caval LN metastasis. (E) The radiofrequency electrode was advanced into the lesion. (F) The CT scan 6 months later showed complete response and no enhancement. (G) The preoperative computed tomography scan showed a retroperitoneal LN metastasis. (H) Absolute alcohol (20ml) was slowly injected into the retroperitoneal LN metastasis. (I) The CT scan 3 months later showed significant tumor shrinkage, complete response and no enhancement.
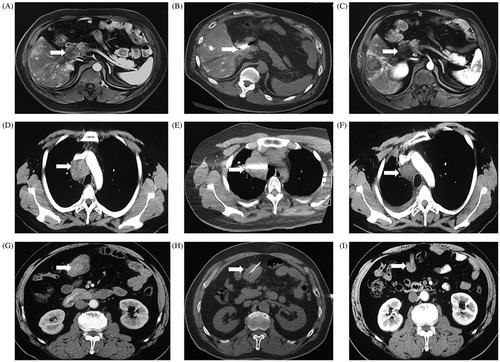
Table 1. The major characteristics of included patients who had lymph node metastases originating from hepatocellular carcinoma.
Table E1. The complete characteristics of included patients who had lymph node metastases originating from hepatocellular carcinoma.
Table 2. The treatment efficacy assessed at 24 h after ablation for lymph node metastases in different sites.
Figure 2. Tumor response after percutaneous ablation therapy based on the Modified Response Evaluation Criteria in Solid Tumor. Abbreviations: CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
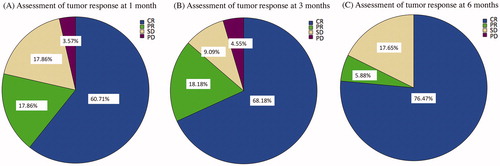
Table 3. The tumor response after ablation therapies for metastatic LNs based on mRECIST criteria.
Figure 3. Survival curves after ablation therapy for treatment of lymph node metastases in patients with hepatocellular carcinoma. (A) The overall survival (OS) rate of patients with lymph node metastases after percutaneous ablation therapy. (B) The local progression - free survival (LPFS) rate of patients with lymph node metastases after percutaneous ablation therapy. (C) The progression-free survival (PFS) rate of patients with lymph node metastases after percutaneous ablation therapy. (D) The OS rates after ablation therapies, including RFA, MWA, and PEI, in patients with lymph node metastases. (E) The LPFS rates after ablation therapies, including RFA, MWA, and PEI, in patients with lymph node metastases. (F) The PFS rates after ablation therapies, including RFA, MWA, and PEI, in patients with lymph node metastases. Abbreviations: RFA, radiofrequency ablation; MWA, microwave ablation; PEI, percutaneous ethanol injection; LNM, lymph node metastases.
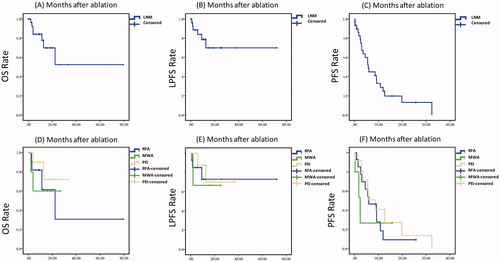
Table 4. The 1-, 2-, 3-, 4- and 5-year OS, PFS, LPFS rates of metastatic lymph nodes after ablation.