Figures & data
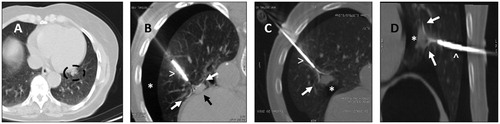
Figure 1. (A, B and C) Lung metastases presentation on CT-scan. Patient with three metachronous, bilateral metastases (arrows) from a rectal cancer. All metastases are sub-pleural, in the lung bases, with well-defined margins. In image B, there is a vessel going into the tumor, this is called ‘the Feeding-Vessel’ sign (arrowhead).
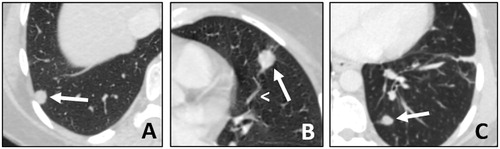
Figure 2. A. 67-y.o. patient with a single metastasis from rectal cancer, 28 mm in diameter, (black asterisk) treated with MWA (white arrow). B. A post treatment pneumothorax was found (white asterisk). C. It required thoracic drain insertion (black arrow). The drain was withdrawn at day 1 and the patient dismissed.
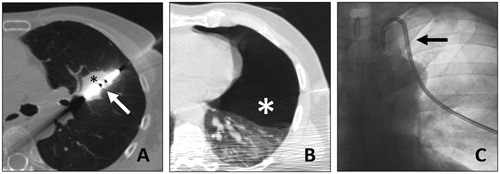
Figure 3. Cryoablation of a posterior right basal lung metastasis with four needles. A. Lung metastasis before treatment (black asterisk). B. Final positioning of the four needles (arrowheads) in the lung lesion (asterisk) in MIP (B(0).1) and VR (B(0).2) reconstructions. C. Lung lesion at the end of the treatment (asterisk) with minimal peripheral intra alveolar hemorrhage (white arrows). D. Control of cryoablation scares (asterisks) at 1 month (D(0).1), 3 months (D(0).2) and 6 months (D(0).3).
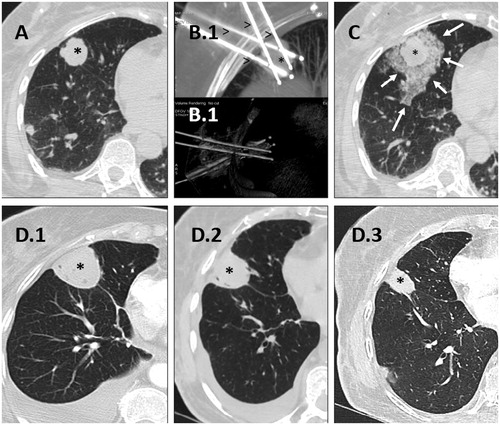
Table 1. Main differences according to ablation technic for lung metastases treatment.
Figure 4. A. Left para cardiac nodule (circle) before treatement with RFA. B. Use of deployable needle (arrowhead) with multiple tips (white arrows) to catch the nodule (black arrow) after performing an artificial pneumothorax (asterisk). C & D. Once the needle tips (white arrows) are deployed in the nodule (asterisk), the probe (arrowhead) is retracted, in order to create a space between the heart bordert and the lesion, to reduce the heat sink effect and avoid major damages to the surrounding structures.