
Figures & data
Figure 1. The IMACTIS-CT® navigation system is composed of a magnetic transmitter attached to the patient’s skin for patient referential (A), a needle holder with an electromagnetic locator (B) and a station with a touch screen (C). The needle used by the operator is equipped with an electromagnetic receiver that detects the position and the orientation of the needle guide and displays the anticipated trajectory of the needle in real-time on two perpendicular 2D reconstructed CT images extracted from the 3D CT volume.
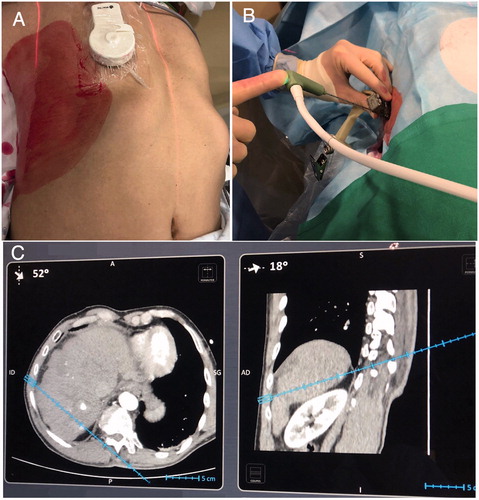
Figure 2. Dynamic T1-weighted MR sequences with contrast administration in arterial (left) and venous (right) phases showed a small (1 cm) segment VIII lesion with typical pattern of HCC, in a cirrhotic patient of 73 year old A. The lesion was not visualized on US and unenhanced CT (left). An intra-arterial hepatic injection of iodized oil (Lipiodol) was performed to make the lesion detectable (right) B. A one-plane trajectory access was impossible on CT-guidance. Therefore, a RF electrode was inserted using EMN and HFJV. A first-pass control CT (coronal reconstructions) was performed before the target had been reached to confirm both the correct path of the applicator and the distance we needed to advance C. The probe was then advanced accordingly on EMN until the target was reached, as confirmed on coronal pre-ablation CT acquisition D. A single ablation was performed and cauterization of the electrode track had been used. Axial post-ablation CT confirmed an ablation area that covered the entire lesions E. Three-month (left) and 6-month (right) contrast enhanced MRI confirmed a complete ablation without residual enhancement F. HCC: hepatocellular carcinoma; CT: Computed Tomography; EMN: electromagnetic navigation; HFJV: high-frequency jet-ventilation; RF: radiofrequency.
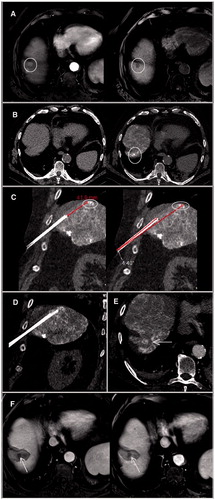
Figure 3. First-pass control CT (coronal reconstruction) acquired after applicator insertion using EMN system and HFJV, for a 4-mm liver metastasis located on the dome, in a 73-year-old man with colon cancer. The needle path was considered adequate to reach the target, with an angle between the needle trajectory and the line connecting the entry point and the center of the lesion of 5.7 degrees; the tip-to-tumor distance was 29 mm A. The probe was then advanced accordingly on EMN. A second control CT showed that the target had been reached B. EMN: electromagnetic navigation; HFJV: high-frequency jet-ventilation; CT: Computed Tomography.
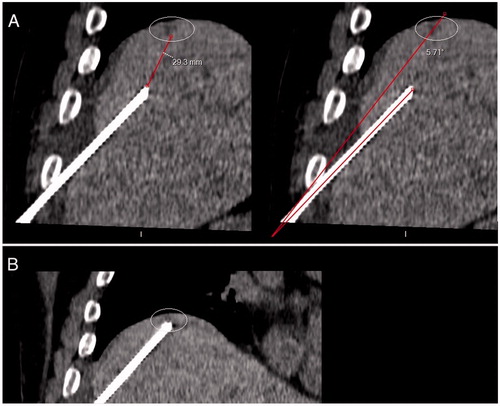
Table 1. Patients and lesions characteristics.
Table 2. Characteristics and results of liver ablations performed for 21 patients with a total of 27 liver tumors.