
Figures & data
Figure 1. Flow chart shows patient selection criteria. The bold sections are the inclusion criteria of MWA. iPTH: intact PTH; MIBI: technetium 99m (99mTc) sestamibi.
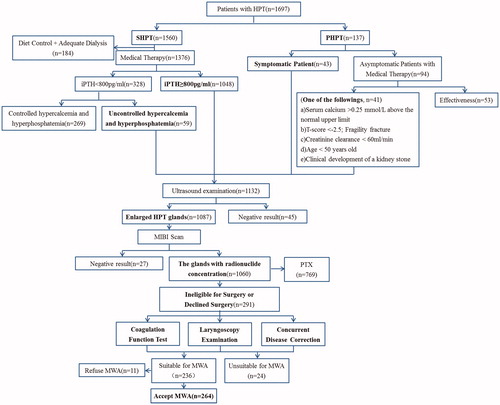
Table 1. Complications and side effects in 264 patients who underwent MWA of HPT.
Table 2. Comparison of relevant clinical parameters between SHPT patients with and without complications.
Figure 2. (a)Transverse US scan in a 69-year-old SHPT patient shows a parathyroid nodule (white arrow) behind inferior left lobe of thyroid abutting the trachea (T) and esophagus (E). (b–c) One and 21 months after MWA, US image shows the shrunken ablation zone(white arrow) clings to the area of the recurrent laryngeal nerve. (d–e) The left vocal cord (white arrow) loses tension, atrophies to be arched and becomes thin under eupnea on US. The left vocal cord is located on one side and could not close the glottis. Laryngoscopy revealed atrophic and thin left vocal cord.
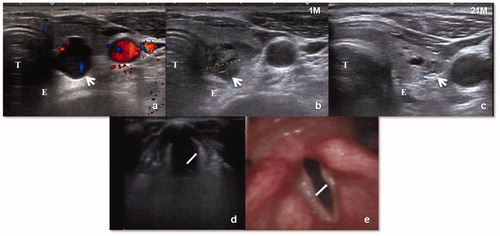
Figure 3. (a) An ectopic parathyroid nodule (white arrow) was on the lateral side of the left carotid sheath. (b) A liquid-isolating zone around the nodule (white triangle). (c) The procedure of MWA. (d) One month after MWA, the nodule showed a reduction in volume on US and the ablation zone (white arrow) was close to middle cervical sympathetic ganglion (MCSG) (yellow arrow).
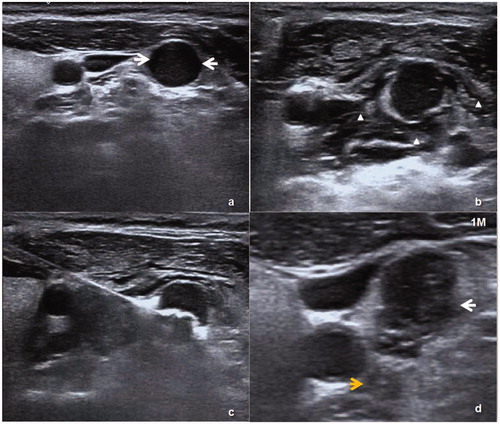
Figure 4. (a) Preablation fingertip necrosis. (b) Seven days later the skin necrosis involved the entire forearm. (c–d) Debridement plus autologous skin transplantation.
