
Figures & data
Table 1. Baseline characteristics of the patients and tumors.
Figure 1. (a) An 18-gauge sheathed needle was inserted into the peritoneal space between the lesion and the risk organs under computed tomography guidance. (b) The inner stylet of the sheath needle was removed, and a 0.035-inch guidewire was inserted through the sheath. (c) A 5-French sheath was introduced into the peritoneal cavity over the guidewire. (d) Sufficient volume of 0.9% saline solution was injected through the sheath to separate the tumors from the risk organs.
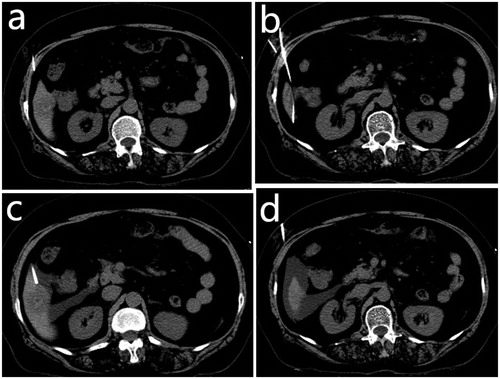
Figure 2. A 65-year-old woman with hepatocellular carcinoma in live segment VI. The patient was treated previously with transcatheter arterial chemoembolization. (a) Contrast-enhanced computed tomography (CT) scan before microwave ablation showed a slightly enhanced lesion with partial lipiodol deposition. The lesion was adjacent to the hepatic flexure of the colon. (b) The electrode needle was inserted into the lesion under CT guidance after the artificial ascites was infused. The lesion was separated from the colon. (c) Contrast-enhanced CT scans obtained immediately after microwave ablation showed complete ablation without enhanced zones in the lesion. (d) No enhancement in the target tumor or peripheral area was observed on the follow-up contrast-enhanced CT 1 month later.
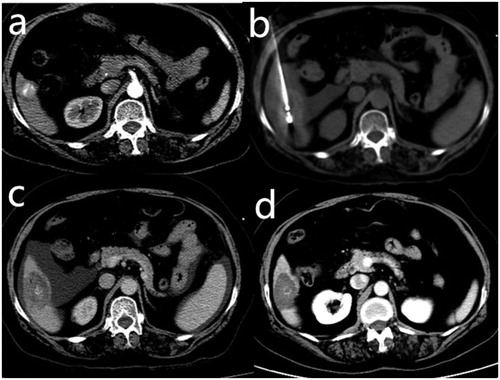
Table 2. Adverse events related to microwave ablation assisted with artificial ascites.