
Figures & data
Table 1. Clinical features of 33 patients with multiple ground-glass opacities (GGOs) and GGO characteristics.
Table 2. Parameters of microwave ablation and the course of treatment in 66 procedures.
Figure 1. A 69-year-old female patient had three synchronous GGOs in three lobes of the bilateral lungs. She underwent two separate MWA procedures with an interval of 1 year. (A, B) GGO lesions (arrow) of 22 mm × 16 mm and 12 mm × 10 mm in the apicoposterior segment of the left upper lobe and in the superior segment of the left lower lobe, respectively were observed on the axial HRCT before MWA. (C) One of the GGOs in the left lung was biopsied and pathologically diagnosed as MIA before MWA. (D, E) MWA was performed on two GGOs in the left lung with an ablation power/time of 60 W/9 min and 60 W/5 min, respectively. (F, G) Reactive fibrous scars with a clear boundary formed at 4 months after MWA (H, I) Further shrinkage of the fibrous scars was visible at 12 months after MWA. (J, K) Only fibrotic streaks were visible at 30 months after MWA. (L) A GGO lesion (arrow) of 14 mm × 11 mm in the posterior basal segment of the right lower lobe was observed on HRCT and pathologically diagnosed as AIS. (M) MWA was performed on the GGO with an ablation power/time of 50 W/7.5 min. (N) Ablated zone of 38 mm × 26 mm was seen at 24 h after MWA. (O) A fibrotic streak formed in the right lower lobe at 18 months after MWA. GGOs: ground glass opacities; MWA: microwave ablation; HRCT: high-resolution computed tomography; MIA: microinvasive adenocarcinoma; AIS: adenocarcinoma in situ.
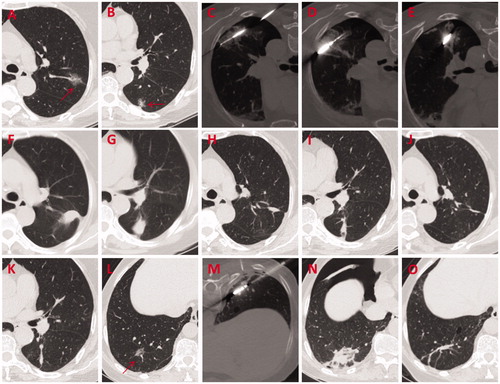
Figure 2. A 61-year-old female patient with two synchronous GGOs in the same lobe underwent MWA procedure for both lesions simultaneously. (A, B) GGO lesions (arrow) of 15 mm × 15 mm and 15 mm × 12 mm located in the posterior basal segment of the right lower lobe were observed on axial HRCT before MWA. (C, D) MWA was performed on two GGOs with an ablation power/time of 40 W/7 min and 65 W/5 min, respectively. (E, F) Ablated zones of 40 mm × 25 mm and 40 mm × 35 mm, respectively were seen at 24 h after MWA. (G–J) Shrinking ablated zones with a denser texture and a clear boundary were observed at 3 months after MWA. (K–N) Non-enhancing coarse fibrotic streaks were visible at 24 months after MWA. GGOs: ground-glass opacities; MWA: microwave ablation; HRCT: high-resolution computed tomography.
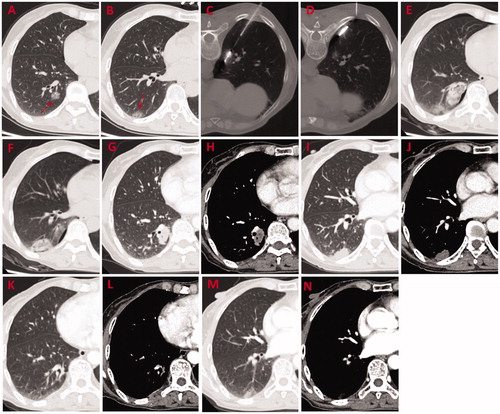
Figure 3. Local progression-free survival and overall survival of all patients.
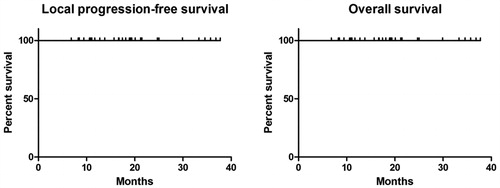
Table 3. Side effects and complications during and after 66 microwave ablation procedures.