
Figures & data
Table 1. Characteristics of 48 patients who underwent thermal ablation for a centrally located renal lesion (n = 58).
Figure 1. Treatment of a left kidney central tumor with renal sinus extension with image-guided microwave ablation and retrograde pyeloperfusion. (a) T1-weighted, fat-saturated, contrast-enhanced MR image demonstrating a centrally located tumor (white arrow) with extension in close proximity of the renal sinus. (b) Retrograde pyeloperfusion was performed through a single j stent (white arrowheads) placed endoscopically the day of the ablation with the tip located in the renal pelvis (white arrow). (c) Microwave antenna (white arrowheads) was inserted under real-time US visualization. (d) CT confirmed the precise positioning of the microwave antenna at the level of the tumor. (e, f) Contrast-enhanced CT 6 months after treatment demonstrates the correct ablation of the tumor (white arrows) with no residual enhancing tumor either in the arterial phase (e, white arrowhead = arterial branch) or the excretory phase (f, white arrowhead = renal calyx). (g) Contrast-enhanced CT in the arterial phase 12 months after the ablation demonstrating complete ablation with tumor shrinkage (white arrow) and no complications.
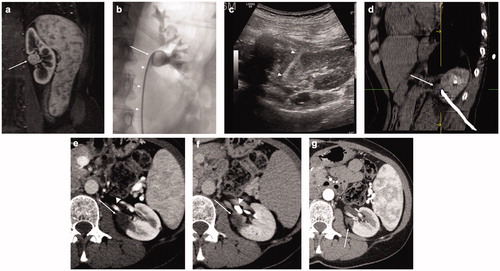
Figure 2. Flowchart of the ablation results (per-lesion analysis). 11 total nephrectomy, 1 active surveillance, 2 untreated due to death of patients for unrelated reasons; 21 total nephrectomy, 3 untreated due to death of patients for unrelated reasons.
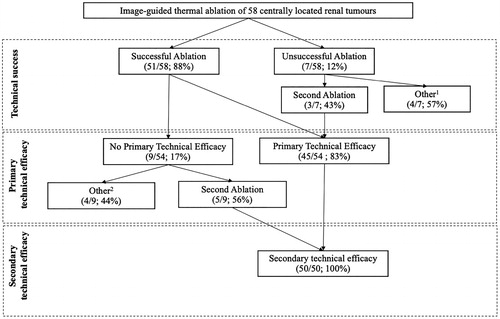
Figure 3. Progression-free survival in a series of 48 patients with kidney lesions treated with thermal ablation. Dashed lines = 95% confidence intervals.
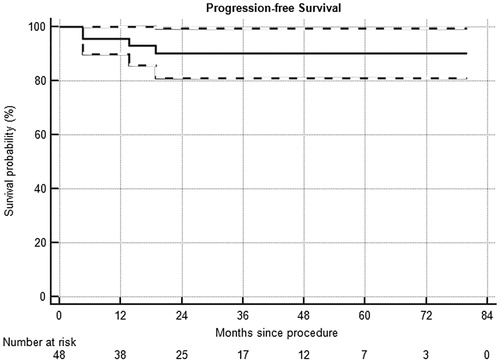
Table 2. Pretreatment and post-treatment characteristics of patients (n = 48) who underwent thermal ablation for a centrally located renal lesion (n = 58).
Table 3. Pretreatment and post-treatment characteristics of mono-renal patients (n = 7) who underwent thermal ablation for a centrally located renal lesion (n = 8).
Table 4. Complications among patients (n = 48) who underwent thermal ablation for a centrally located renal lesion (n = 58), classified according to SIR standards [Citation17].