
Figures & data
Figure 1. CBCT-guided lung RFA with virtual guidance in a 62-year-old woman. (a) CT image shows an 8-mm nodule (arrow) in the left lower lobe. (b) Virtual-guided planning for a safe needle route (green line) to the target lesion was performed. (c) When CBCT moves automatically until the entry-point view (i.e., vertical alignment from the entry site [red circle] to the target lesion [green circle] with virtual color), spots can be seen on the fluoroscopic image. (d) CBCT was performed after electrode placement to confirm the exact location of the needle tip.
![Figure 1. CBCT-guided lung RFA with virtual guidance in a 62-year-old woman. (a) CT image shows an 8-mm nodule (arrow) in the left lower lobe. (b) Virtual-guided planning for a safe needle route (green line) to the target lesion was performed. (c) When CBCT moves automatically until the entry-point view (i.e., vertical alignment from the entry site [red circle] to the target lesion [green circle] with virtual color), spots can be seen on the fluoroscopic image. (d) CBCT was performed after electrode placement to confirm the exact location of the needle tip.](/cms/asset/89049946-3be7-498b-91d9-e4121e61bfdb/ihyt_a_1784472_f0001_c.jpg)
Figure 2. Workflow followed in our study from pre-procedural CBCT to management of complication.
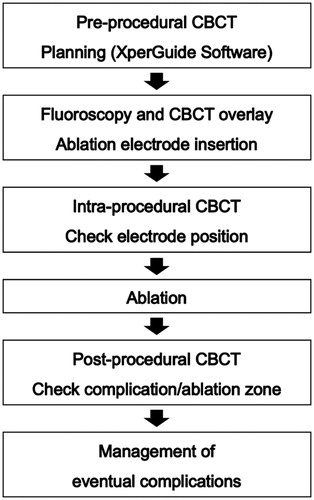
Table 1. Characteristics of the 100 RFA sessions in 63 patients with a total of 121 tumors.
Table 2. Major Complications in 100 Lung Radiofrequency Ablation (RFA) Sessions.
Figure 3. An 81-year-old man underwent RF ablation of pulmonary metastasis from colorectal carcinoma in the anterior basal segment of the right lower lobe. (a) Chest CT obtained before RFA shows the tumor (arrow), which demonstrates the intimate relation of central pulmonary lesions with the blood vessels, thereby increasing the risk of pulmonary hemorrhage. (b) CBCT image during insertion of RF electrode. Notice traversing the intervening pulmonary vessels by the needle electrode. (c) C-arm fluoroscopy image showed the extent of intra-parenchymal hemorrhage after the insertion of the electrode. Immediate termination of the ablation session was decided because of excessive hemoptysis and deterioration of the clinical condition of the patient. The patient was treated in the intensive care unit. (d) After 3 h, progressive increase in pulmonary hemorrhage was observed in chest plain radiography.
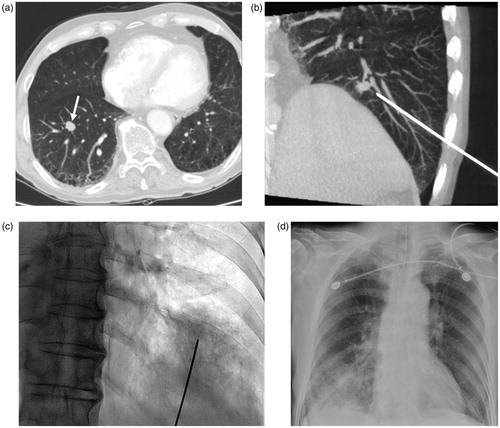
Figure 4. Bronchopleural fistula developed after lung radiofrequency ablation in a 34-year-old woman with an intrapulmonary metastasis from ovarian cancer. (a) Chest CT obtained before RFA demonstrates the tumor (arrow) in the right middle lobe. (b) There is an electrode placement through the tumor under CBCT guidance. (c, d) Computed tomography image obtained 51 days after ablation shows collection of fluid and air (arrowhead) in the right major fissure and adjacent bronchus (arrow), suggesting the possibility of bronchopleural fistula. (e) Plain chest radiograph obtained 82 days after ablation shows large pneumothorax. The bronchopleural fistula was closed after surgical repair.
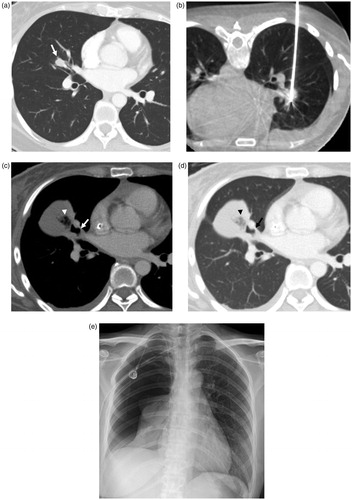
Table 3. Minor Complications in 100 Lung Radiofrequency Ablation (RFA) Sessions.