Figures & data
Table 1. Radiofrequency ablation parameters by internally cooled electrode tip size using the optimized pulse algorithm.
Figure 1. Short course, large volume RF ablation with long term favorable outcome. (a) A 2.2 cm HCC at S8 (arrow) was ablated with a single insertion of a 4 cm exposed tip RF electrode in 6 min with 2000 mA current. (b) At 24-h, CT the dimensions of the necrosis volume achieved were 4.8 × 4.3 × 5.5 cm. At 2- (c) and 4-year (d) follow-up, ablation was complete with no LTP.
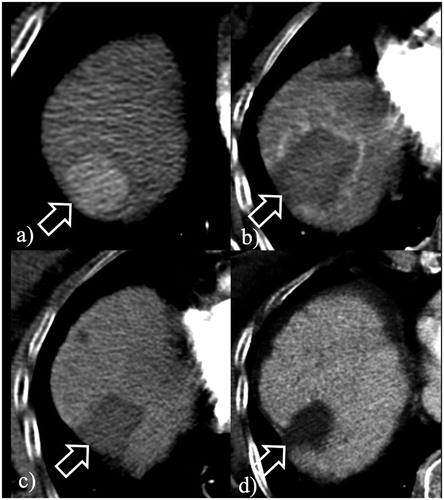
Figure 2. Large volume RF ablation from optimized current and longer electrodes. (a) A 4.2 cm HCC at S4 (arrow) was ablated with a single insertion of a 4 cm exposed tip RF electrode in 12 min with 2200 mA current. (b) At 24-h CT, the dimensions of the necrosis volume achieved were 5.2 × 4.1 × 4.4 cm. (c) At 2-year follow-up, ablation was complete with no LTP.
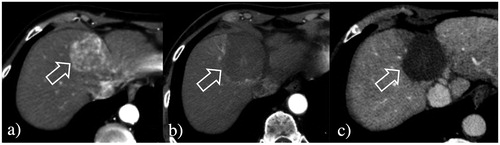
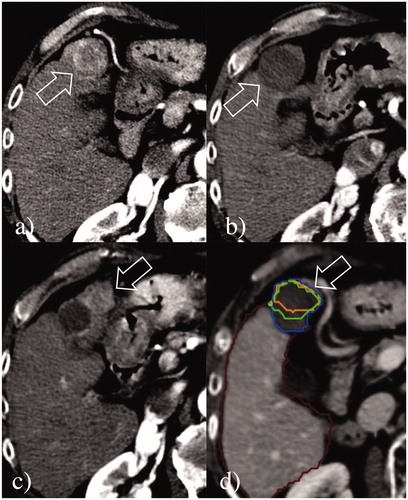
Figure 3. Local tumor progression post-RF ablation from incomplete treatment. (a) A 3.3 cm HCC at S4 (arrow) was ablated with a single insertion of a 3 cm exposed tip RF electrode in 6 min with 1600 mA current. (b) At 24-h CT, the dimensions of the necrosis volume achieved were 3.5 × 3.3 × 3.5 cm. (c) Although the treatment seemed to be complete, at 9-month follow-up CT, a large region of local tumor progression was noted in the anterior portion of the volume of necrosis (arrows). (d) Retrospective assessment of the pre- and post-ablation CT scans non-rigidly co-registered by Ablation-fit software (RAW s.r.l., Milan, Italy) showed that a small portion (15.4%) of the 5-mm ablative margin (green line) was not achieved in the anteromedial part of the HCC, suggesting incomplete treatment was due to an initial technical failure from sub-optimal electrode placement and ablation coverage. The margins of the volume of necrosis (blue line), of the HCC (orange line), and the ablative margin are exactly overlapping.