
Figures & data
Figure 1. Flow chart of selection patients.
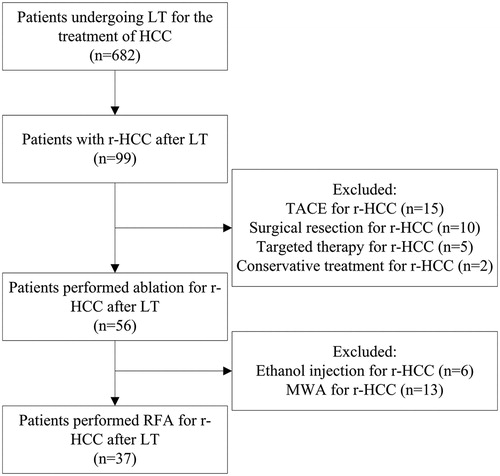
Table 1. The baseline characteristics of the patients.
Table 2. The location and treatment for limited EM.
Figure 2. Images in a 60-year-old man received radiofrequency ablation (RFA) for a recurrent hepatocellular carcinoma (r-HCC) in the transplanted liver. A, Pre-interventional B-mode ultrasound showed a tumor sized 1.5 cm × 1.4 cm (arrow). B and C, Contrast-enhanced ultrasound (CEUS) before RFA showed obvious enhancement in the artery phase (B) and washout in the late phase (C) (arrow). D and E, Contrast-enhanced computed tomography (CECT) before RFA showed obvious enhancement in the artery phase (D) and washout in the late phase (E) (arrow). F, Electrode placement during the ablation (arrowhead). G, Tumor appeared completely hyperechoic after the beginning of RFA. H, CEUS obtained 1 month after RFA showed no contrast enhancement, suggesting complete ablation.
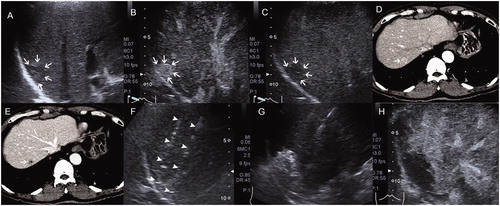
Table 3. The details of the patients with incomplete ablation after the first session of RFA.
Figure 3. Local tumor progression in patients performed RFA for r-HCC after liver transplantation.
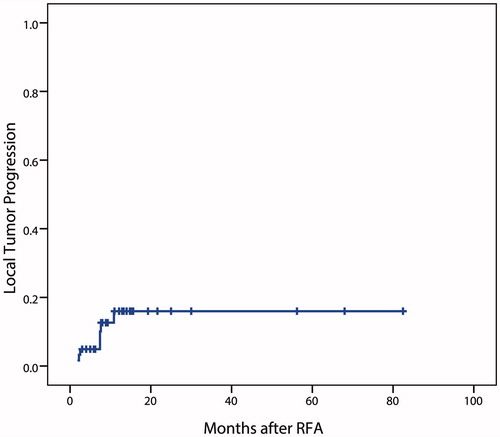
Figure 4. Recurrence-free survival in patients performed RFA for r-HCC after liver transplantation. A, in all patients; B, comparison between patients with maximum tumor diameter ≤ 3 cm and > 3 cm.
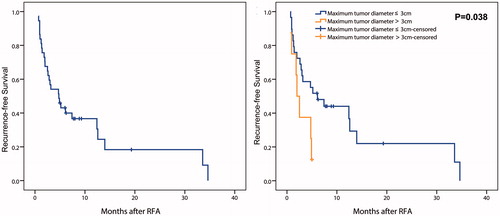
Table 4. Prognostic factors of RFS in patients performed RFA for r-HCC after LT.
Figure 5. Overall survival in patients performed RFA for r-HCC after liver transplantation. A, in all patients; B, comparison between patients with and without limited extrahepatic metastasis.
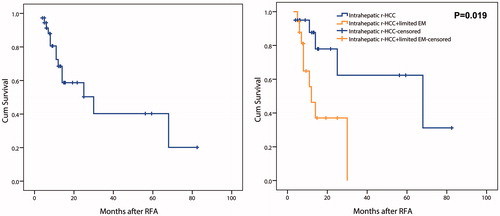
Table 5. Prognostic factors of OS in patients performed RFA for r-HCC after LT.