
Figures & data
Figure 1. Study flow-chart.
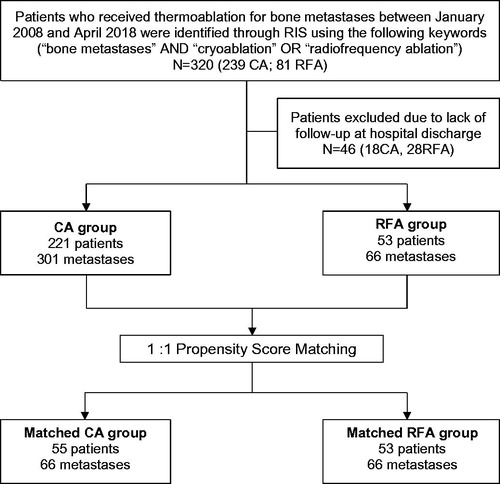
Figure 2. Curative cryoablation of a solitary scapular metastasis of a papillary thyroid cancer in a 63-year-old male patient. Axial Short Tau Inversion Recovery (STIR) (A) and coronal T1 weighted (T1W) contrast enhanced (B) MR acquisitions (A, B) show the metastatic lesion of the scapular spine (white arrows). Multiplanar reconstructed CT images (C) display the positioning of 4 cryoprobes along the long axis of the lytic lesion (white arrows). Axial CT image (D) shows the maximal iceball (arrow heads); in this case, the supraspinatus muscle was hydrodissected (black arrow). A hydrodissection of the suprascapular nerve was also performed with a 22 G needle placed in the suprascapular notch (not shown). In this patient, a symptomatic post-ablation fracture occurred 1 month after the procedure as shown on coronal CT reconstructions (arrows in E). This fracture was treated by percutaneous screw fixation (arrows in F).
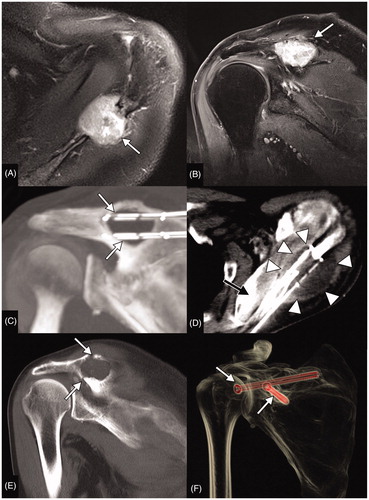
Figure 3. Palliative bipolar radiofrequency ablation of an L3 lung cancer metastasis in a 67-year-old male complicated with early post-procedural spondylodiscitis and para vertebral abscess. Sagittal T1W (A) and STIR (B) acquisitions show enlargement of the metastatic infiltration of the L3 vertebral body (arrowhead); there were also benign vertebral compression fractures of the adjacent vertebral bodies (arrows). Pre,-procedural CT (C) shows the lysis of the L3 body (arrow) but also enlargement of the left psoas muscle (arrowheads) secondary to soft tissue metastasis. Per procedural fluoroscopic (D, E, F) and CT (G) images show the positioning of the RF electrodes (white arrows), an 18 G epidural needle (black arrow) allowing dissection of the epidural space (black arrow in G) and the final acquisition prior to needle removal and after cementoplasty of L3 and the adjacent fractured vertebra (F). Contrast-enhanced axial T1W (H) and axial T2W (I) acquisitions obtained 3 d after the procedure show an abscess within the left psoas muscle communicating with the L2/L3 disk (arrows).
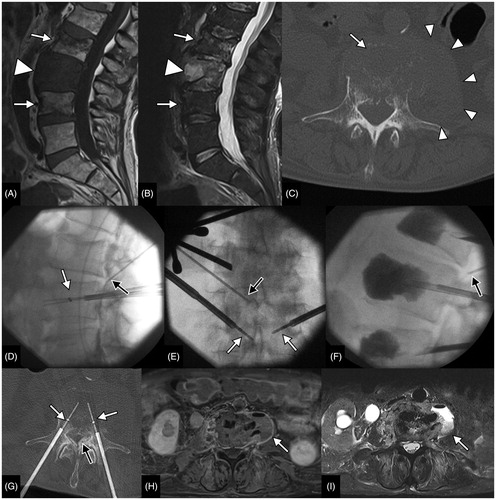
Table 1. Patient demographics and tumor characteristics in the entire unmatched population.
Table 2. Major complications in the entire unmatched population according to the applied thermal ablation technique.
Table 3. Minor complications in the entire unmatched population according to the applied thermal ablation technique.
Table 4. Patient demographics and tumor characteristics in the 1:1 matched population.
Table 5. Analgesic protocol recently adopted at authors’ institution.