
Figures & data
Figure 1. Patient selection flow diagram / Patients who had (a) serum prostate-specific antigen (PSA) levels ≤ 20 ng/mL, (b) prostate cancer (PC) detected using transrectal ultrasound (TRUS)-guided target and systematic transrectal biopsy, (c) T stage: T1c-T2c, (d) life expectancy longer than 10 years, (e) no metastasis, (f) no severe anal strictures, and (g) no previous history of treatment for PC were informed of the procedure as an optional treatment. In addition to the standard treatment, those who underwent high-intensity focused ultrasound (HIFU) provided informed consent. Neo-adjuvant therapy (NHT) was recommended for patients who were diagnosed with high-risk PC or had prostate volume of ≥ 40 cc, or had over 6 months until the treatment schedule. NHT was performed for the patients who agreed to the use of NHT after they provided informed consent, which provided information regarding the possibility of adverse effects of NHT for 6 to 12 months before HIFU. Compression methods were recommended for patients with prostate volume ≤ 25 cc because of the ease of prostatic swelling during the treatment, and informed consent, which provided information regarding the possibility of rectal injury, was performed. For patients with prostate volume > 25 cc, the compression method was informed as an optional treatment technique. The compression method was performed for patients who agreed to undergo the novel treatment technique.
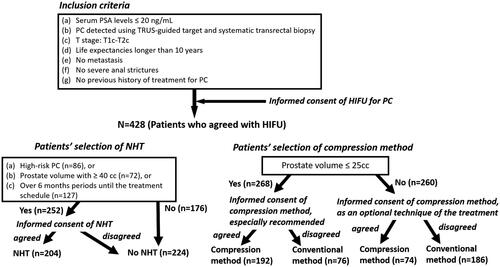
Figure 2. Biochemical disease-free survival of the patients who were treated with high-intensity focused ultrasound over a median follow-up period of 5 years / The biochemical disease-free survival of the patients who were treated with high-intensity focused ultrasound for localized prostate cancer in the total, low-, intermediate-, and high-risk groups according to D’Amico risk groups were 68.4, 80.4, 65.6 and 61.6%, respectively, over a median follow-up period of 5 years.
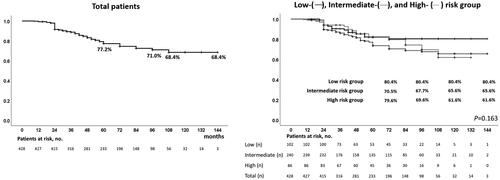
Figure 3. Biochemical disease-free survival of patients treated with high-intensity focused ultrasound with and without neo-adjuvant hormonal therapy over a median follow-up period of 5 years / In patients treated with high-intensity focused ultrasound for localized prostate cancer, disease-free survival in patients with and without neoadjuvant hormonal therapy showed no significant difference in total (74.9 and 58.3%, p = 0.194), low- (84.5 and 76.1%, p = 0.446), and intermediate-risk groups (71.6 and 55.1%, p = 0.469), but there was a significant difference in the high-risk group (79.0 and 43.7%, p = 0.027) over a median follow-up period of 5 years.
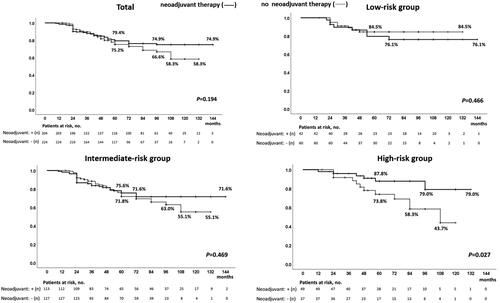
Figure 4. Biochemical disease-free survival of patients treated with high-intensity focused ultrasound with and without the compression method over a median follow-up period of 5 years / In patients treated with high-intensity focused ultrasound for localized prostate cancer, disease-free survival rates in patients treated with and without compression were significantly different in total (78.6 and 51.3%, p < 0.0001) and in low- (88.2 and 59.3%, p = 0.002), intermediate- (77.2 and 49.5%, p < 0.0001), and high-risk groups (67.1 and 48.9%, p = 0.006) over a median follow-up period of 5 years.
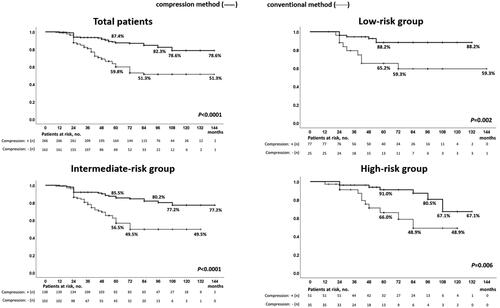
Figure 5. Biochemical disease-free survival of patients treated with high-intensity focused ultrasound without neo-adjuvant hormonal therapy with and without the compression method over a median follow-up period of 5 years / In patients treated with high-intensity focused ultrasound for localized prostate cancer, biochemical disease-free survival in patients without neo-adjuvant hormonal therapy with and without compression methods were significantly different in total (64.9 and 49.9%, p < 0.0001) and in low- (93.2 and 62.3%, p = 0.027), intermediate- (59.5 and 53.7%, p = 0.013), and high-risk groups (50.1 and 30.0%, p = 0.047) over a median follow-up period of 5 years.
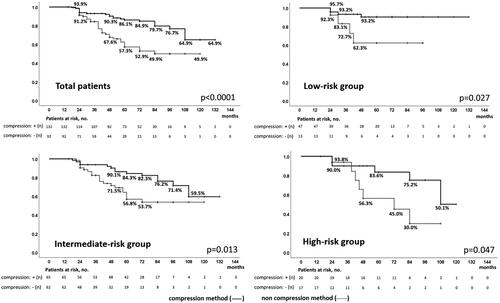
Figure 6. Biochemical disease-free survival of patients treated with high-intensity focused ultrasound with neo-adjuvant hormonal therapy with and without the compression method over a median follow-up period of 5 years / In patients treated with high-intensity focused ultrasound for localized prostate cancer, biochemical disease-free survival in patients who underwent neoadjuvant hormonal therapy with and without compression was significantly different in total (87.0 and 52.5%, p < 0.0001) and in low- (85.2 and 58.3%, p = 0.051), and intermediate-risk groups (86.7 and 43.9%, p < 0.0001), but not in the high-risk group (84.1 and 72.6%, p = 0.056) over a median follow-up period of 5 years.
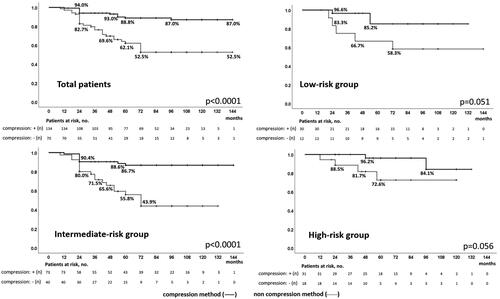
Figure 7. Rates of three-dimensional measured volume of disappearance of blood flow in each prostate gland / The rates of three-dimensional measured volume of disappearance of blood flow were significantly higher in patients diagnosed with non-recurrence than in the low- (89 vs. 74%, p < 0.0001), intermediate- (88 vs. 68%, p < 0.0001), and high-risk groups (90 vs. 64%, p < 0.0001). Furthermore, the rates of the three-dimensional measured volume of disappearance of blood flow were significantly higher in patients treated with the compression method than with the conventional method in patients with recurrence and non-recurrence in the low- (p < 0.0001 and p = 0.001), intermediate- (p < 0.0001 and p < 0.0001), and high- (p < 0.0001 and p = 0.003) risk groups.
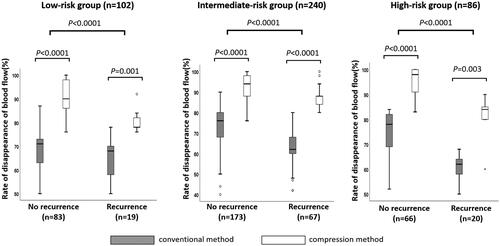
Table 1. Patient characteristics.
Table 2. Perioperative data.
Table 3. Comparison of characteristics of patients treated with and without neo-adjuvant hormonal therapy.
Table 4. Comparison of characteristics of patients treated with and without compression method.
Table 5. Comparison of characteristics of patients diagnosed as having biochemical failure and no failure after the treatment.
Table 6. Comparison of characteristics of patients diagnosed as having biochemical failure and no failure after the treatment according to D’Amico risk groups.
Table 7. Univariate and multivariate logistic regression analyzes to predict biochemical failure after the treatment according to D’Amico risk groups.
Table 8. Complications in patients treated with the compression and conventional methods.
Table 9. IIEF-5 score in the all patients over 12 months after the treatment (n = 428).
Table 10. IIEF-5 score in patients with erectile function before the treatment over 12 months after the treatment (n = 179).