
Figures & data
Figure 1. CONSORT flow diagram summarizes the patient enrollment process in this study.
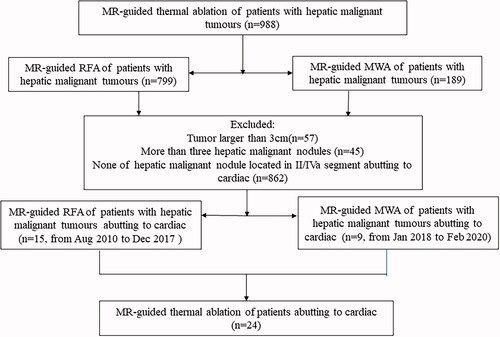
Table 1. Patients’ characteristics.
Figure 2. Recurrent HCC in the hepatic dome abutting to heart of a 55-year-old woman treated with MR-guided RFA. (A,B) The recurrent nodule in segment IV (arrow), 3 mm from pericardium, is 7 mm in diameter and appears hypointense in T1WI before RFA. (C) The recurrent nodule is displayed unclearly on plain CT scan. (D) The RF electrode is targeted gradually using the tilting of the puncture path under the coronal 3D-T1WI guidance. When the RF electrode reaches the edge of the nodule, the inner expandable multitined electrodes are expanded to 2.0 cm to overlap the nodule without penetrating the diaphragm. (E–G) After RFA, the nodule is completely overlapped by the rim of the hyperintensity on 3D-T1WI and hypointensity on T2WI (arrow in G). (H,I) The lesion is completely ablated without diaphragm and heart injury at 4-month follow-up by enhanced MRI.
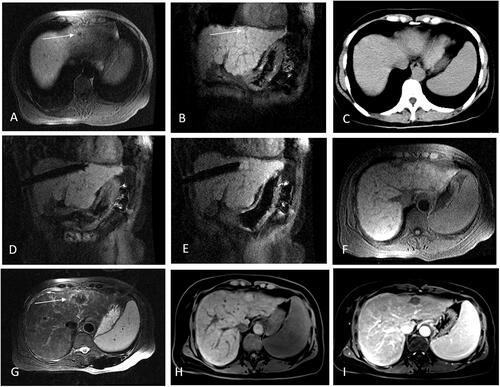
Figure 3. Recurrent HCC after liver resection in the hepatic dome abutting to heart of a 35-year-old man treated with MR-guided MWA. (A,B) The recurrent nodule 4.8 mm from pericardium,13 mm in diameter of segment II appears hyperintense in T2WI and hypointense in T1WI before MWA. (arrow in A,B). (C,D) The MW antenna is gradually targeted and inserted under the coronal T2WI, and the relationship between the antenna and heart is clearly displayed in coronal image. (E–G) A typical ‘target sign’ (arrow) is clearly shown in the ablative zone with the hypointense nodule completely overlapped by the hyperintensity on 3D-T1WI and hypointensity on T2WI, with a safe margin immediately after MWA and without diaphragm and heart injury. (H,I) The ablative zone with the ‘target sign’ is completely ablated without enhancement in MRI at 1-month follow-up.
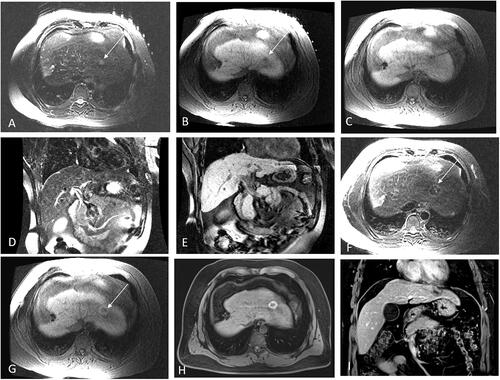
Figure 4. Probability of LPFS and estimated OS in 24 patients with 25 hepatic malignant lesions located on segment II or IVa abutting the heart (mean diameter: 13.4 ± 6.3 mm, range: 7–30 mm), treated with Mrguided thermal ablation after a median follow-up of 28 months. (A) Graph showing 1-, 3-, and 5-year LPFS rates as 100%, 94.7%, and 94.7%, respectively. (B) Graph showing the estimated 1-, 3-, and 5-year OS rates as 91.7%, 80.6%. and 50.1%, respectively.
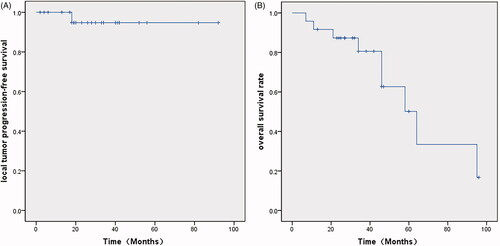
Table 2. Incidence of complications related to ablation.