
Figures & data
Figure 1. Representative case showing the usefulness of the multiple-electrode switching system radiofrequency ablation (MESS-RFA) in ablating a large volume at one time. (A) Image before MESS-RFA showing. A 3.5-cm nodule (arrowheads) with enhancement in the arterial phase. (B) Intra-procedural contrast-enhanced ultrasound guiding tumor (arrowheads) targeting and monitoring. (C) Axial CT image immediately after MESS-RFA showing that the ablation zone (arrowheads) covers the index tumor (5.5 cm in size). (D) Coronal CT image reconstructed from the immediate post-procedural CT scan shows that the ablation zone (arrowheads) measures 5.4 cm in its coronal long axis.
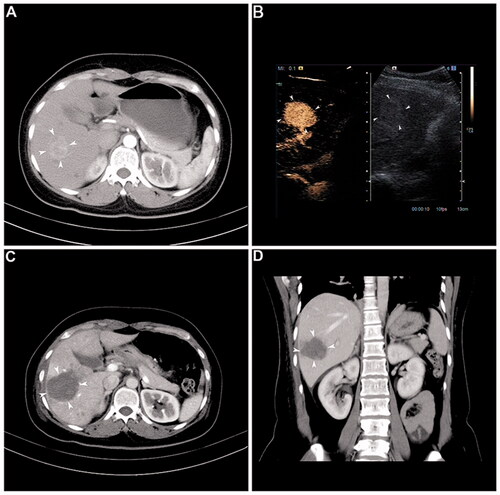
Figure 2. The flow chart shows the first-line treatment results for 139 HCC patients who met the Milan criteria and were treated with a multiple-electrode switching system radiofrequency ablation (MESS-RFA).
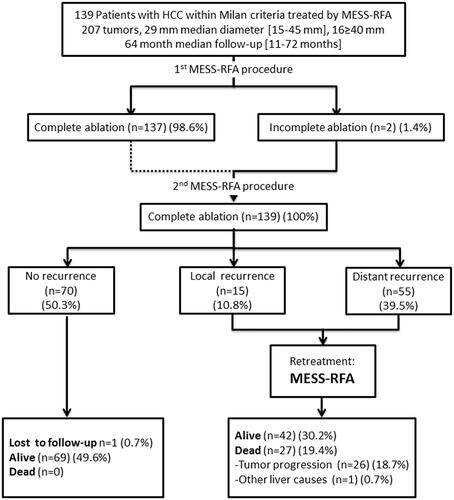
Table 1. Baseline characteristics of the 139 patients with HCC treated by percutaneous MESS-RFA.
Figure 3. The overall recurrence-free survival curve. Sixty-nine patients (49.7%) out of the 139 patients were found to have intrahepatic recurrence (LTP and/or IDR) during follow-up. These recurrences occurred 60 months after ablation (ranging from 3 to 72 months).
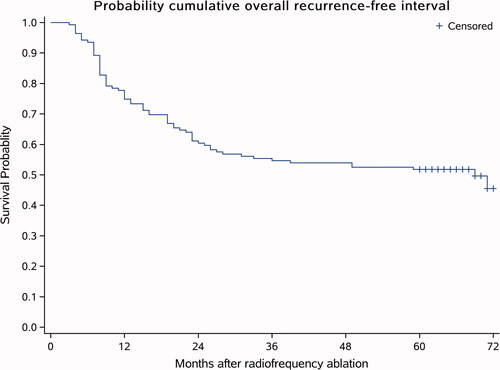
Table 2. Risk factors for LTP in univariate and multivariate analysis.
Figure 4. IDR-free survival curve. Fifty-five (39.56%) patients out of the 139 patients had IDR, and the estimated 1-year, 3-year and 5-year IDR-free survival rates were 78.75, 61.79 and 60.17%, respectively. The average follow-up time was 64 months (ranging from 11 to 72 months).
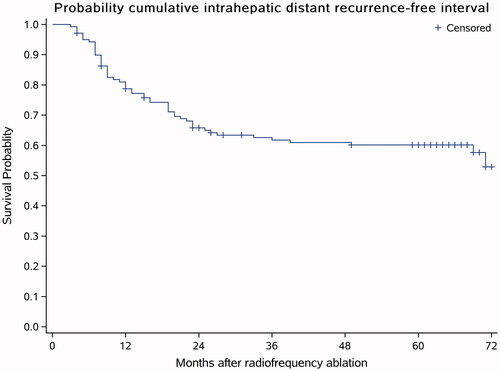
Table 3. Risk factors for IDR in univariate and multivariate analysis.
Figure 5. Overall survival curve. The average follow-up time was 59.33 ± 15.34 months, the median follow-up time was 64 months, and 1 patient was lost to follow-up after 24 months. During the follow-up, 27 (19.42%) people died. Among the 27 dead patients, the deaths of 26 patients (18.70%) were associated with HCC progression and one patient (0.71%) had gastric fundus hemorrhage.
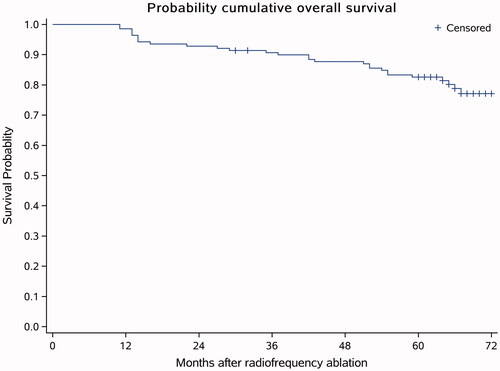
Table 4. Risk factors for overall survival in univariate and multivariate analysis.
Table 5. Comparison of the recurrence time and different survival states.