
Figures & data
Figure 1. Octopus MP electrode system.
A. Two 17-gauge internally cooled electrodes with adjustable active tip lengths at 5-mm intervals (ICAE) (electrodes with longer needle shafts) and one 19-gauge multipurpose needle (MPN) capable of temperature monitoring and adjuvant agent injection (needle with shorter shaft). B. Adjustment of the active tip length in an ICAE. C. The MPN tip with four 0.3-mm-sized side holes (arrowheads a and b) and a thermometer (arrowhead c). Below is the schematic diagram of cross sections at each corresponding arrowhead level.
T: thermometer.
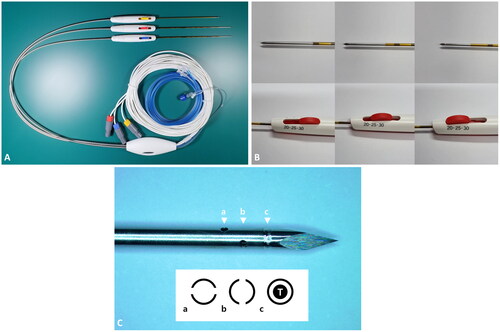
Figure 2. Schematic diagram of the multipurpose needle (MPN) strategy.
For the usual cases, the MPN is inserted into the tissue between margin of the tumor and the external margin of ablation zone in order to monitor adequacy of treatment temperature ①. For adjuvant injection (AI), the MPN is inserted into the parenchyma near the tumor margin where the operator plans to create a larger ablation zone ②. For subcapsular parenchyma temperature monitoring (SPTM), the MPN is inserted into the subcapsular parenchyma for continuous temperature monitoring to avoid thermal injury in nontarget organs ③. For all MPN insertions, special care was taken not to directly puncture the tumor for oncological safety purposes.
E: electrode.
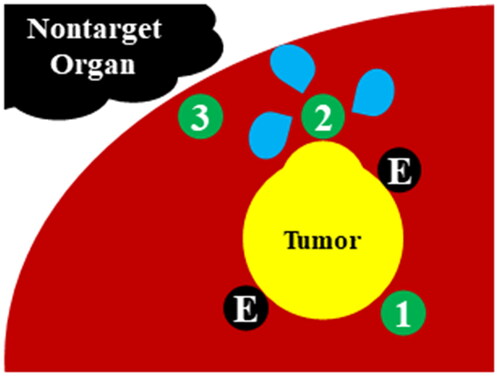
Table 1. Baseline characteristics of patients, tumors, and ablation procedures.
Table 2. Treatment outcomes.
Figure 3. Changes in current, impedance, and temperature before, during, and after adjuvant saline infusion in two cases with adjuvant injection (AI).
In both cases, the temperature (monitored by the MPN) dropped sharply at the beginning of the saline infusion. However, the saline infusion did not affect the impedance and current (monitored by the ICAEs) meaningfully in both cases.
MPN: multipurpose needle; ICAE: internally cooled electrode with adjustable active tip length.
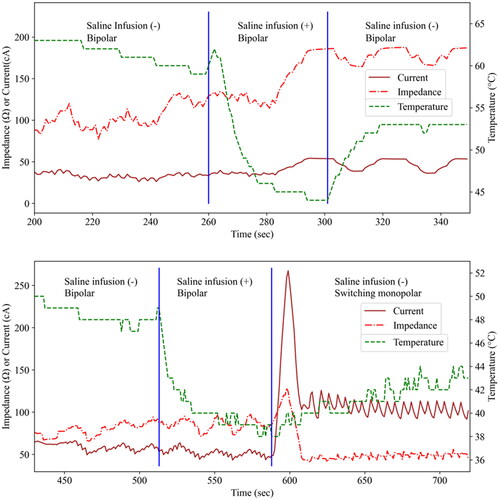
Figure 4. Successful ablation of a subcapsular tumor with nearby hepatic flexure of the colon in a 57-year-old male patient.
A 1.3-cm subcapsular tumor with hepatobiliary phase defect (arrowhead, upper left) and mild T2 hyperintensity (arrowhead, upper right) is close to the hepatic flexure of the colon. With US-MR fusion guidance, two ICAEs were inserted into the peritumoral parenchyma in a parallel manner with an interelectrode distance of 2.0 cm (middle left). An MPN was inserted into the subcapsular parenchyma (arrows, middle right) for SPTM. Note that the hepatic flexure of the colon lies close to the peritumoral liver capsule even after artificial ascites infusion (asterisk, middle right). In the immediate (lower row) and one-month follow-up CT (not shown), the index tumor was surrounded by an ablation zone with sufficient margin (arrowhead, lower left). Nontarget injuries were not observed in the colon (asterisk, lower right) and other nearby structures.
ICAE: internally cooled electrode with adjustable active tip length; MPN: multipurpose needle; SPTM: subcapsular parenchyma temperature monitoring; CT: computed tomography.
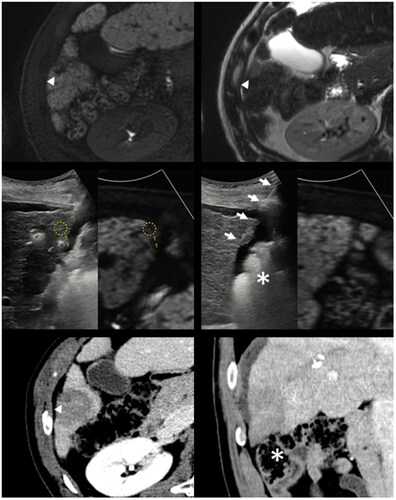
Figure 5. Technical Failure with a residual unablated tumor in a 69-year-old male patient.
A 0.4-cm-sized arterially enhancing nodule (arrowhead, upper left) with portal phase washout (arrowhead, upper right) was not visualized on B-mode ultrasound. RFA was performed under US-CT fusion guidance (arrow and arrowhead, middle left). In the immediate follow-up CT, nodular arterial phase enhancement (arrowhead, middle right) with portal phase washout (arrowhead, lower left) was noted but was mistakenly interpreted as a part of a treatment-related hyperemic rim. In the one-month follow-up CT, residual unablated tumor tissue is clearly delineated (arrowhead, lower right).
RFA: radiofrequency ablation; CT: computed tomography.
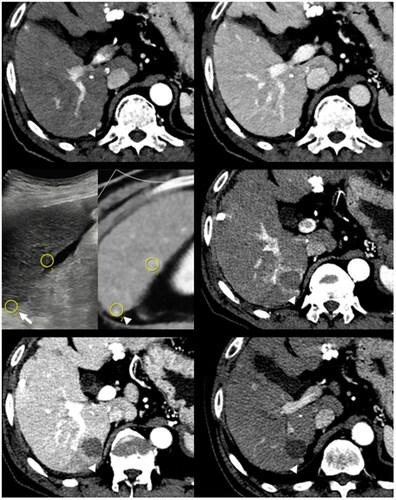
Table 3. Utility of the novel adjustable electrodes and multipurpose needles.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author, Jeong Min Lee. The data are not publicly available due to the privacy of research participants.