
Figures & data
Figure 1. Pelvic magnetic resonance image of a type II–Ⅵ uterine fibroids. (A) Sagittal view of the T2-weighted image reveals the fibroid located in the posterior wall and fundus of the uterus, extending more than 50% into the muscular layer. (B) Transverse images demonstrate the fibroid on the posterior wall protruding into the uterine cavity, with an anteroposterior diameter of 8 cm.
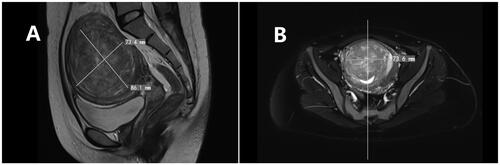
Figure 2. Hysteroscopic image of a single type II–Ⅵ fibroid before and after HIFU. (A) Preoperative hysteroscopy shows that 20% of the fibroid protrudes into the uterine cavity. (B) On the second day after HIFU, hysteroscopy reveals that 60% of the fibroid now protrudes into the uterine cavity.
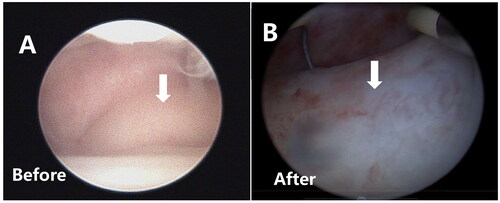
Table 1. STEPW classification scoring system.
Table 2. Score and treatment recommendations according to STEPW classification scoring system.
Figure 3. Contrast-enhanced ultrasound image obtained from a patient with a solitary type II–Ⅵ fibroid. (A) Pre-HIFU contrast-enhanced ultrasound showed significant perfusion of the fibroid. (B) Post-HIFU contrast-enhanced ultrasound showed no perfusion of the fibroids. The fibroid was completely ablated.
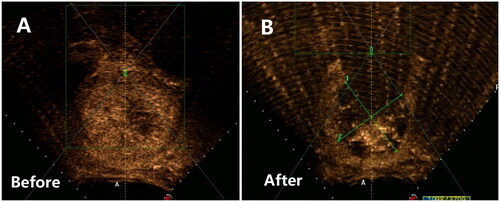
Table 3. Comparison of baseline characteristics between the two groups of patients.
Table 4. Comparison of intraoperative conditions between HIFU + HM group and HM group.
Table 5. Comparison of pre- and post-HIFU STEPW scores in the HIFU + HM group
Table 6. Comparison of myomectomy rate between the two treatment methods n (%).
Table 7. PBAC score before and after HM treatment or after HIFU + HM treatment.
Table 8. PBAC score before and after the two treatment methods, health-related quality of life questionnaire for uterine fibroids (UFS-QOL form).
Table 9. Statistics of complications of treatment methods in the two groups n (%).
Data availability statement
The data that support the findings of this study are available upon request from the corresponding author, TTL. The data are not publicly available because it contains information that can compromise the privacy of the research participants.