Figures & data
Table 1. Subjects and their demographic data.
Table 2. Detection ratio of each chemokine in tears by performing beaded assay.
Figure 1. Determination of chemokine levels in tears by using the magnetic bead assay. Tear levels of CCL17/TARC (A), CCL24/eotaxin-2 (B), and IL-16 (C) in patients with AKC and VKC are significantly higher than those in patients with AC; *p < 0.05, **p < 0.01. AC: allergic conjunctivitis, AKC: atopic keratoconjunctivitis, VKC: vernal keratoconjunctivitis, TARC: thymus and activation-regulated chemokine, IL-16: interleukin-16, ND: not detected.
Table 3. Partial correlation coefficient of patients with AKC and VKC.
Figure 2. Correlation between eosinophil cationic protein (ECP) and eotaxin-2 levels in the tears of patients with atopic keratoconjunctivitis (AKC) and vernal keratoconjunctivitis (VKC). Tear levels of ECP were determined by chemiluminescent enzyme immunoassay and those of eotaxin-2 were determined by magnetic bead assay. Significant correlation was observed between ECP and eotaxin-2 levels in the tears of patients with AKC (n = 6) and VKC (n = 14) (Spearman rank correlation coefficient, ρ = 0.68, p < 0.005).
Figure 3. Clinical scores of patients with AC. Clinical scores of patients with AC were determined using the 5-5-5 exacerbation scale.
a. Clinical scores of patients with AC treated with epinastine ophthalmic solution significantly decreased after 7 days compared with those at baseline (p < 0.001, Wilcoxon signed rank test).b. Patients with AC were divided into 3 groups based on their treatment outcomes: patients showing improvement (n = 12), patients showing immutability (n = 5), and patients showing exacerbation (n = 0).
Figure 4. Tear levels of IL-16 and eotaxin-2 in patients with AC. In patients with AC showing improvement (n = 12), tear levels of IL-16 decreased significantly 7 days after the treatment compared with those at baseline (p < 0.05, Wilcoxon signed rank test). Similarly, tear levels of eotaxin-2 decreased at 7 days after the treatment compared with those at baseline. However, statistical significance could not be calculated due to a small sample size.
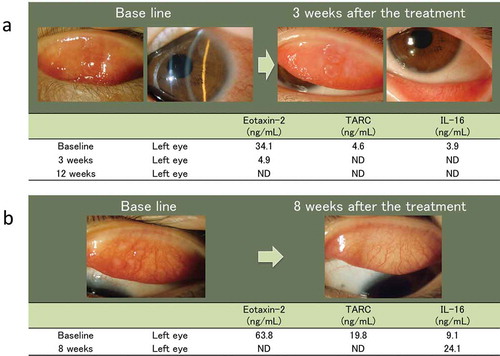
Figure 5. Clinical features of 2 patients with VKC, and the results of the tear cytokine/chemokine test in these patients.
a.An 8-year-old girl with VKC. Slit-lamp photographs showing several giant papillae in the upper tarsal conjunctiva and diffuse thickening of the limbal tissue, with trantas spots in both eyes at baseline. These clinical observations improved and tear levels of CCL17/TARC and CCL24/eotaxin-2 decreased after treatment with 2% sodium cromoglycate and 0.1% cyclosporine ophthalmic solution.b.An 8-year-old boy with VKC. Slit-lamp photographs showing several giant papillae in the upper tarsal conjunctiva in both eyes. These clinical observations improved and tear levels of CCL17/TARC and CCL24/eotaxin-2 decreased after treatment with 0.5% tranilast and 0.1% cyclosporine ophthalmic solution. ND: not detected.