Figures & data
Figure 1. Intervention schematic. Automated dose reminders prompt patients to check in to the mobile application and submit a video of each prescribed inhaled corticosteroid dose (dark blue). The emocha platform facilitates encrypted transmission of uploaded patient videos to a secure server for remote review by study nurses (video DOT). Nurses assess patient adherence and inhaler technique during video DOT (medium blue). Patients receive personalized feedback via the in-app chat function (light blue); nurses can also communicate with patients via phone call or escalate issues to the patient’s pediatrician, and patients can initiate chat communication with nurses for on-demand support.
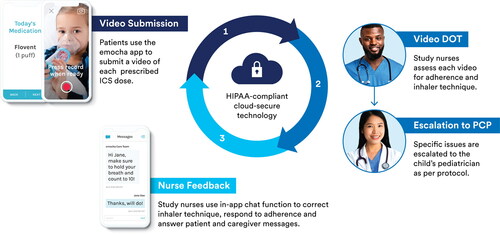
Figure 2. Study flow and analysis cohorts. Of 26 eligible patients, 24 enrolled. Of these, 21 submitted at least one video and comprised the overall cohort used for the feasibility analysis. Participants with adequate program engagement (participated >7 days and submitted >4 videos) were included in the analysis of preliminary program outcomes (inhaled corticosteroid adherence and inhaler error rate). A total of eight participants (2 patients and 6 adult caregivers) could be reached for the telephone interview at the end of the program and contributed qualitative data on feasibility, acceptability and user satisfaction.
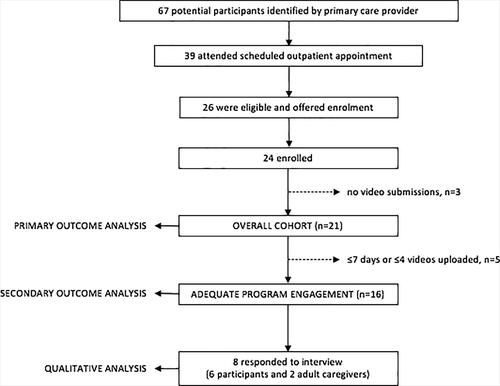
Table 1. Baseline characteristics among enrolled children with poorly controlled asthma by analysis cohort.
Figure 3. Descriptive trends in (A) primary and (B) secondary outcomes by program week. Feasibility (A), as measured by program engagement, decreased over the first four weeks; 57% of enrolled children remained engaged at week 5, and median program adherence decreased from 64% to 50% over the first three weeks. Those that remained engaged past week 4 tended to complete the program and maintain higher program adherence. (B) During the first two weeks, over 90% of patients with adequate engagement submitted videos (grey bars), median inhaled corticosteroid adherence remained above 80% (dashed line) and inhaler technique improved with resolution of most errors (solid line).
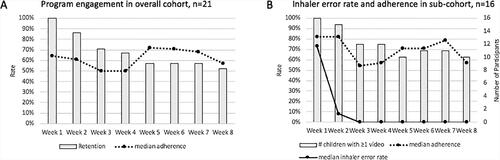
Figure 4. Inhaler errors and adherence issues detected in the overall cohort (n = 21). Among 810 video submissions, nurses detected 247 inhaler errors and 107 adherence issues. (A) Errors in breath holding, forgetting to shake the inhaler before use and taking an adequate breath in were most common among children in our cohort. The majority of adherence issues were behavioral barriers (B), particularly disrupted routines and forgetfulness. The most common medication administration issue (C) was taking more or less drug than prescribed
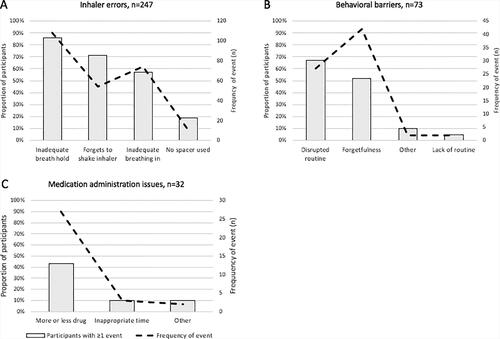
Table 2. Qualitative interview themes categorized according to study outcome (n = 8 respondents; two participants and six caregivers).a
Figure 5. Change in inhaler technique during the first three weeks in children with adequate engagement (n = 16). The box and whisker plot (A) summarizes inhaler errors by program week, illustrating significantly improved inhaler technique from week 1 to week 2 (median error rate 73% [IQR 18–85] vs 8% [IQR 0–50], p < 0.05). (B) Each colored line represents one participant. The majority of children (14 of 16, 88%) demonstrated improved inhaler technique over the first 3 weeks, as measured by proportion of videos with at least one error; one child made more errors over time, and one child maintained error-free technique throughout the program. Colors indicate three major patterns: orange indicates immediate resolution of most errors (error rate < 20%) within one week (6 of 16, 38%); blue indicates more gradual improvement with resolution of most errors by week 3 (5 of 16, 31%); and the green line indicates either consistently low (<20%) or high (>80%) error rate (4 of 16, 25%).
![Figure 5. Change in inhaler technique during the first three weeks in children with adequate engagement (n = 16). The box and whisker plot (A) summarizes inhaler errors by program week, illustrating significantly improved inhaler technique from week 1 to week 2 (median error rate 73% [IQR 18–85] vs 8% [IQR 0–50], p < 0.05). (B) Each colored line represents one participant. The majority of children (14 of 16, 88%) demonstrated improved inhaler technique over the first 3 weeks, as measured by proportion of videos with at least one error; one child made more errors over time, and one child maintained error-free technique throughout the program. Colors indicate three major patterns: orange indicates immediate resolution of most errors (error rate < 20%) within one week (6 of 16, 38%); blue indicates more gradual improvement with resolution of most errors by week 3 (5 of 16, 31%); and the green line indicates either consistently low (<20%) or high (>80%) error rate (4 of 16, 25%).](/cms/asset/3a63a11f-788c-40b3-88d5-9d840374e72d/ijas_a_1984525_f0005_c.jpg)
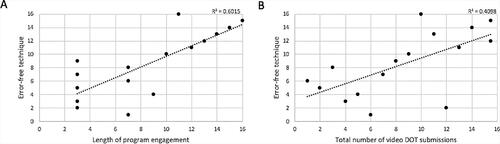
Figure 6. Relationship between program engagement and correct technique using Spearman’s rank order correlation (rs) in children with adequate engagement (n = 16). Correct technique was quantified as the proportion of video submissions with error-free technique. Scatter plots show (A) a strong positive correlation between length of program engagement and error-free technique (rs = 0.776) and (B) a moderate positive correlation between total number of video submissions and error-free technique (rs = 0.640).