Figures & data
Figure 1. A 58 year old woman with metastatic thyroid cancer. Euthyroid (left panel), hyperthyroid due to functioning mediastinal metastases (middle panel), and euthyroid after thyroidectomy and 131I treatment and on thyroid hormone substitution (right panel).

Figure 2. Profile scanning of 131I uptake showing initial uptake over metastases in the mediastinum. After 131I treatment uptake in the thyroid rest is observed. After retreatment with 131I also the thyroid rest is ablated.
Figure 3. A 67 year old woman with thyroid cancer and a skeletal metastasis in the forehead.

Figure 4. Scanning of 131I uptake showing the accumulation in the thyroid and the metastasis.
Figure 5. The patient in , 19 months after thyroidectomy, 131I treatment, external radiotherapy and thyroid hormone substitution.

Figure 6. Scanning of 131I uptake in a 42 year old woman with thyroid cancer operated with right-sided hemithyroidectomy (left panel). The right panel shows uptake in lymph node metastases on the right side of the neck and in the mediastinum following 131I treatment.
Figure 7. Profile scanning of the same patient as in .
Figure 8. Whole body scanning of 131I uptake in a 52 year old man with metastatic thyroid cancer. Metastases to the liver, the lungs and the skeleton are demonstrated.
Figure 9. Liver metastasis of thyroid cancer (compare scan in ).
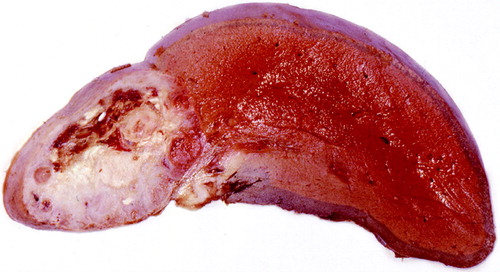
Figure 10. Demonstration of the epilation caused by 131I treatment of a metastasis in the skull (left panel). The right panel shows later regrowth of hair.
Figure 11. Chest radiography showing two pulmonary metastases in a 38 year old woman with thyroid cancer.
Figure 12. The same patient as in after hypophysectomy demonstrating regression of the metastases.
Figure 13. Diagram showing the initial very slow progression of two pulmonary metastases and then the effect of hypophysectomy (compare & ).