Figures & data
Figure 1. Illustration of study design At first visit, metastases were numbered and measured. Data were then brought to an external unit (the pharmacy) who randomized and mixed calcium chloride and bleomycin into syringes labeled with numbers according to the metastases. At treatment, the blinded contents of the syringes were injected intratumorally and followed by electroporation. It was a once-only treatment and the patients were followed for 6 months with regular evaluation of tumor response and safety.
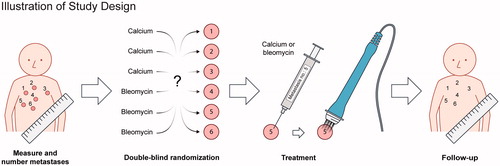
Table 1. Patients demographics.
Table 2. Metastases used for response evaluation.
Figure 2. Tumor response Metastases were treated at day = 0 with either i.t. calcium or i.t. bleomycin in a randomized double-blinded study design. The metastases were treated once only and after 6 months of follow-up, the randomization code was revealed. A. Change in diameter over time: The graph illustrates change in largest diameter over time for metastases treated with calcium chloride (red) and bleomycin (blue) (mean and standard deviation). The three non-measurable metastases treated with bleomycin were not included. B. Percent change in tumor size 6 months after treatment: The graph illustrates a clear difference in tumor response when subdivided into irradiated (CR = 46%) and non-irradiated (CR = 81%) metastases. The three non-measurable metastases treated with bleomycin were non-irradiated, and are not illustrated in the graph, but included in the calculation. C. Percent metastases without progression: The graph illustrates progression in treated metastases after treatment. After 6 months, 11% (2 out of 18) metastases treated with calcium had progressed, and 15% (3 out of 19) metastases treated with bleomycin had progressed. D. Highest measured current: The graph illustrates that there is no significant difference in measured current between bleomycin and calcium (p = 0.5), but a significantly higher delivered current in non-irradiated metastases (light grey) compared to irradiated metastases (dark grey) (p < 0.0001).
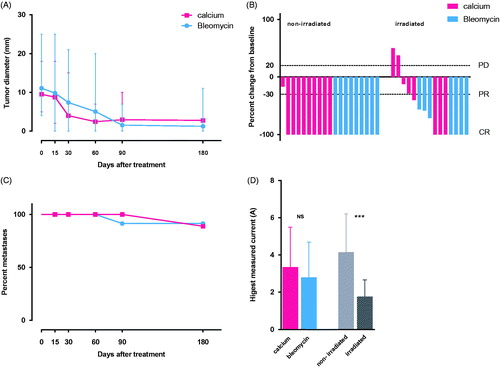
Figure 3. Punch biopsies before and one week after treatment. A–C: Patient no. 3, with nine metastases from breast cancer on the right nates. A: Pre-treatment biopsy: Skin biopsy with a moderate amount of tumor infiltration (black arrow) and fibrosis within the dermis. There is mild inflammation and no necrosis. B: Day 7. Post-treatment with calcium electroporation: Ulcerated skin biopsy with the same amount of tumor infiltration as in the pretreatment biopsy and moderate fibrosis. There is no inflammation or necrosis. C: Day 7. Post-treatment with electrochemotherapy: Ulcerated skin biopsy with no evidence of tumor but a large amount of necrosis (grey arrow) and fibrosis and with mild inflammation. D–F: Patient no. 5 with ten metastases from breast cancer on her left breast and abdomen. D: Pre-treatment biopsy: Skin biopsy with extensive tumor infiltration, moderate fibrosis and minimal inflammation. No evidence of necrosis. E: Day 7. Post-treatment with calcium electroporation: Skin biopsy with less tumor infiltration than in the pretreatment biopsy and a moderate amount of necrosis and fibrosis. There is minimal inflammation. F: Day 7. Post-treatment with electrochemotherapy: Skin biopsy with moderate tumor infiltration, necrosis and fibrosis. There is minimal inflammation.
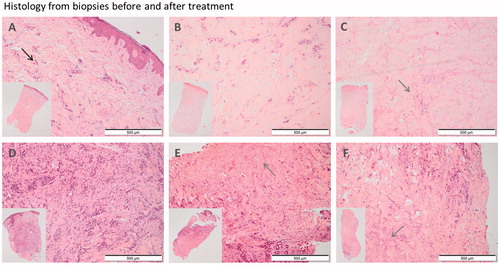
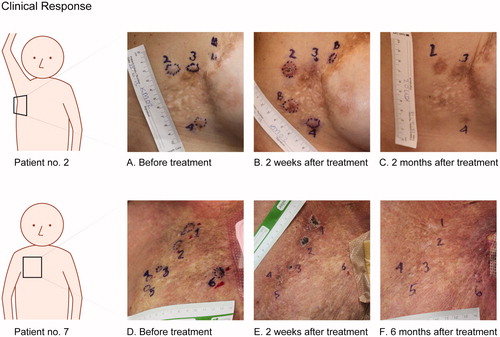
Figure 4. The top row show pictures from patient no. 2 with cutaneous metastases from breast cancer. Metastases 2 and 3 were treated with bleomycin and electroporation, metastasis 4 were treated with calcium and electroporation. The two metastases labeled B were treated with bleomycin outside of protocol. A. before treatment. B. Two weeks after treatment, shows crust on metastases no. 2, disappearing of metastases no. 3, and no visible chance in metastasis no. 4. C. Two months after treatment, show clear hyperpigmentation equivalent to the area treated with bleomycin (metastases no. 2 and 3) and no change in pigmentation in the area treated with calcium (metastases no. 4). Bottom row show pictures from patient no. 7 with cutaneous metastases from breast cancer. Metastases 1–3 were treated with bleomycin and electroporation and metastases 4–6 were treated with calcium and electroporation. D. before treatment. E. Two weeks after treatment, illustrates typical crust appearance, note the ulcer is not extending tumor margin. F. Six months after treatment, shows complete disappearance of metastases 1–5 and no change in metastasis no. 6.