Figures & data
Table 1. Characteristics of the NCCN high-risk cSCC cohort (n = 300).
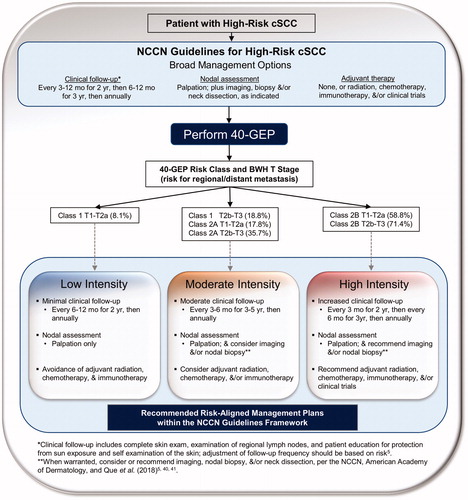
Figure 1. Application of 40-GEP test results to NCCN-defined high-risk status and T stage for improving risk-appropriate management of cSCC. (A) Using a cohort (n = 300) of clinicopathologically-defined cSCC patients meeting study criteria and who were NCCN-defined high risk, the 40-GEP test stratified the patients into three groups depending on risk for metastasis at 3 years post-diagnosis: low (Class 1, n = 189), high (Class 2A, n = 87), or highest (Class 2B, n = 24). Patients stratified as Class 1, 2A, and 2B had a 9%, 21%, and 63% risk for metastasis, respectively, per the 40-GEP test alone. Corresponding AJCC8 and BWH T stages and metastasis rates were analyzed. (B) Incorporation of 40-GEP Class plus AJCC8 and BWH T stages into three metastasis risk bins (<10%, 10–49%, and ≥50% risk) resulted in low, moderate, and high intensity management strategies. The 40-GEP integration demonstrates low management intensity for 53.0% (AJCC8) or 57.7% (BWH), high intensity management for 8.0%, and moderate intensity management for the remainder (39.0%, AJCC8; 34.3%, BWH) of the 300-patient cohort. (C) Metastasis-free survival (MFS) rates of patients from the cohort risk-aligned with low, moderate, or high intensity management per 40-GEP Class and AJCC8 or BWH T stage. Kaplan–Meier analysis revealed 3-year MFS rates of 92.5% for patients in the low intensity management category (both AJCC8 and BWH), 82.1% and 80.6% for those in the moderate intensity category (AJCC8 and BWH, respectively), and 41.7% for patients in the high intensity category (both AJCC8 and BWH). Statistically significant differences were found for these MFS curves for both 40-GEP Class plus AJCC8 and 40-GEP Class plus BWH T stage (p ≤ .001, log-rank).
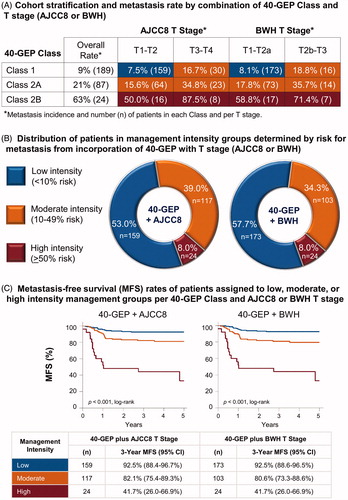
Figure 2. Recommended risk-aligned cSCC patient management plans within the NCCN guidelines framework for prognostic groups based on 40-GEP Class and T stage. Risk for regional/distant metastasis is reported for 40-GEP Class and BWH T stage. *Adjustment of clinical follow-up should be based on risk per the NCCN guidelines. **Imaging, nodal biopsy, and/or neck dissection should be considered (moderate intensity management) or recommended (high intensity management) when warranted per the NCCN, American Academy of Dermatology, and Que et al.Citation41.