
Figures & data
Figure 1. PRISMA flowchart of literature selection.
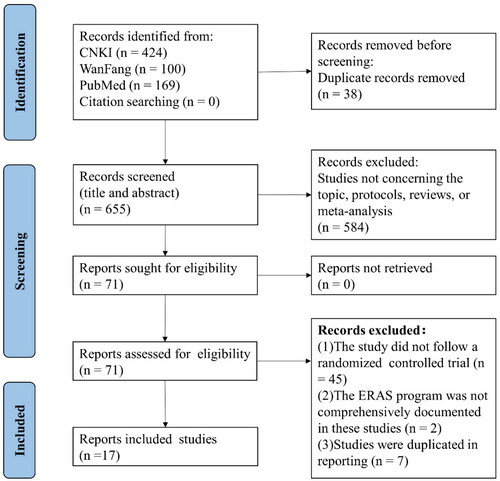
Figure 2. The reporting results of ERAS items in the included RCTs.
(The ERAS items: 1, Preoperative nutrition; 2, Wound catheters and transversus abdominis plane block; 3, Avoid nasogastric/nasojejunal decompression; 4, Avoiding the use of abdominal drains; 5, Early postoperative diet and artificial nutrition; 6, Preoperative counselling; 7, Preoperative smoking and alcohol consumption; 8, Avoid preoperative bowel preparation; 9, Preoperative fasting and preoperative treatment with carbohydrates; 10, No Preanesthetic Medication; 11, Antithrombotic prophylaxis; 12, Antimicrobial prophylaxis and skin preparation; 13, Epidural analgesia; 14, Intravenous analgesia; 15, Anaesthetic management; 16, Prevention of nausea and vomiting; 17, Avoiding hypothermia; 18, Postoperative glycaemic control; 19, Fluid balance; 20, Early urinary drainage tube removal; 21, Stimulation of bowel movement; 22, Early and scheduled mobilization)
Figure 2 showed the ERAS items reported in both the ERAS and TC groups during different time periods: (A) all, (B) before 2015, (C) after 2015.

Table 1. Basic characteristics of the included RCTs.
Table 2. Number of ERAS items adopted in the included RCTs.
Figure 3. The risk of bias graph and risk of bias summary.
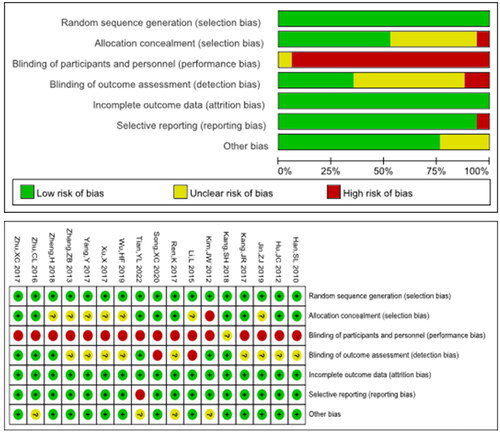
Table 3. Results of the meta-analysis comparing the efficacy between the ERAS group and TC group.
Table 4. Results of the meta-analysis comparing the safety between the ERAS group and TC group.
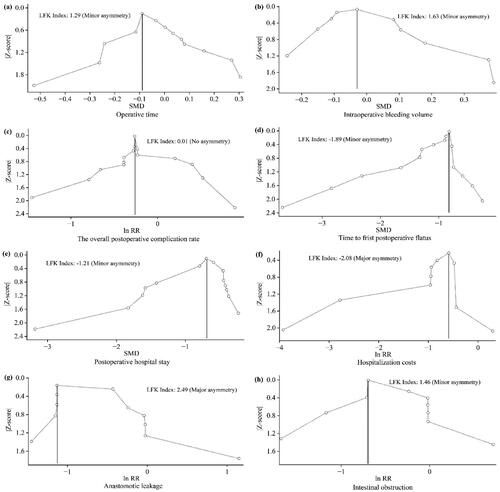
Figure 4. Summary of the Doi plots for each outcome.
Figure 4 showed that publication bias was assessed by Doi plots for each outcome, and asymmetry was indicated using the LFK index for eight outcomes: (a) Operative time, (b) Intraoperative bleeding volume, (c) The overall postoperative complication rate, (d) Time to first postoperative flatus, (e) Postoperative hospital stay, (f) Hospitalization costs, (g) Anastomotic leakage, (h) Intestinal obstruction.
Supplemental Material
Download MS Word (37.7 KB)Data availability statement
Authors of included studies should be contacted individually for further details.