Figures & data
Figure 1 The cardiovascular continuum in hypertension and the relative preventive effect of blood pressure lowering and the ancillary actions of antihypertensive agents. In the therapeutic continuum, the size of the letters indicates the relative and changing importance of the various approaches at various stages of the cardiovascular disease continuum. IGT, impaired glucose tolerance; LVH, left ventricular hypertrophy; IMT, carotid intima‐media thickening; TIA, transient ischaemic attack; MI, myocardial infarction; CHF, congestive heart failure; ESRD, end‐stage renal disease. Adapted from references 2 and 3.
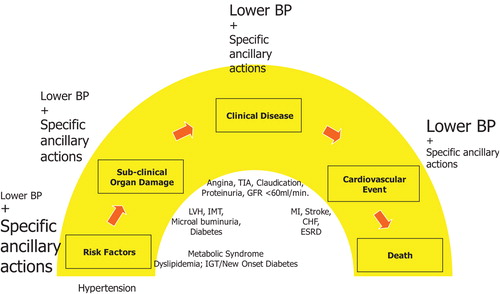
Table I. Risk factors/markers for both cardiovascular disease and chronic kidney disease.
Figure 2 Algorithm for cardiovascular and renal protection in patients with chronic kidney disease and estimated glomerular filtration rate⩾50 ml/min. *Exercise caution over the use of high doses of diuretics. If a beta‐blocker is prescribed, then it should be combined with a DHP CCB. **Carvedilol is preferred because of specific data in renal impairment and outcomes. Other beta‐blockers are not excluded, there are no data to support the use of atenolol in such patients and only limited data to support metoprolol, which is also poorly tolerated. eGFR, estimated glomerular filtration rate; BP, blood pressure; ARB, angiotensin II receptor blocker; ACEI, angiotensin‐converting enzyme inhibitor; CCB, calcium‐channel blocker; DHP CCB, dihydropyridine calcium‐channel blocker.
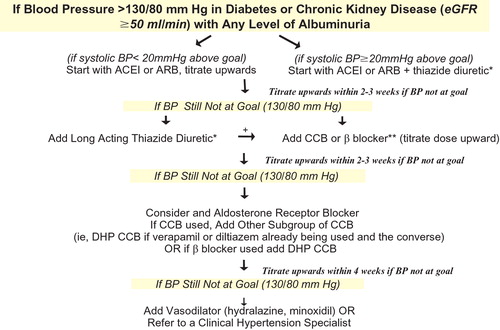
Figure 3 Algorithm of urine spot testing for microalbuminuria to be followed in every patient with chronic kidney disease or elevated cardiovascular risk of apparently other origin. Alb/Cr, albumin/creatinine ratio; GFR glomerular filtration rate.
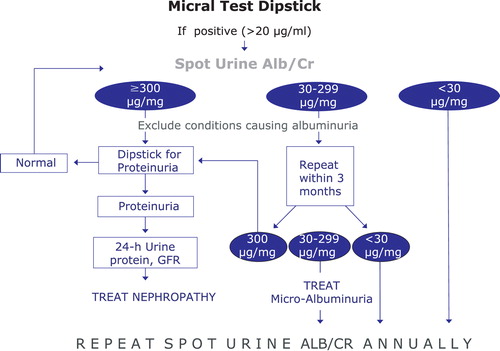
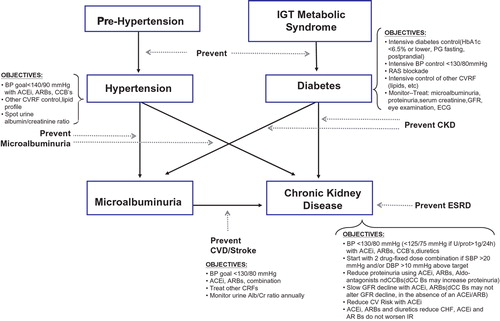
Figure 4 The relationship between hypertension, diabetes and chronic kidney disease and treatment objectives. IGT, impaired glucose tolerance; PG, plasma glucose; BP, blood pressure; RAS, renin–angiotensin system; CVRF, cardiovascular risk factor; GFR, glomerular filtration rate; ECG, electrocardiogram; CKD, chronic kidney disease; ESRD, end‐stage renal disease; ACEI, angiotensin‐converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium‐channel blocker; CVD, cardiovascular disease.