Figures & data
Table 1. Characteristics of patients with resistant hypertension at baseline.
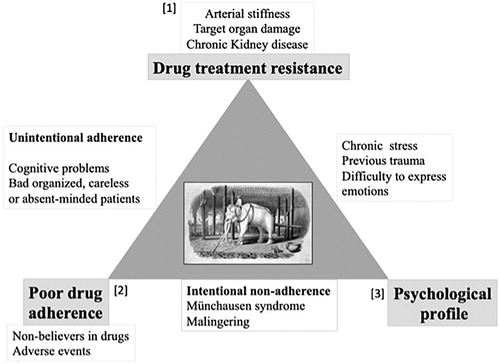
Figure 1. Changes in antihypertensive drugs prescription from baseline to follow-up in the overall cohort of resistant hypertensive patients. *p-Value <0.001. RAS: Renin-Angiotensin-System; FU: Follow-up; CCBs: Calcium Channel Blockers; TZD: Thiazide diuretics.
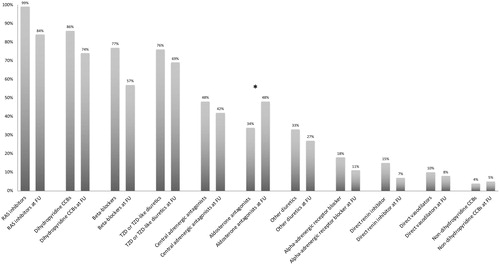
Figure 2. Office and ambulatory BP changes between baseline and follow-up in persistent resistant and controlled hypertensive at follow-up. SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure.
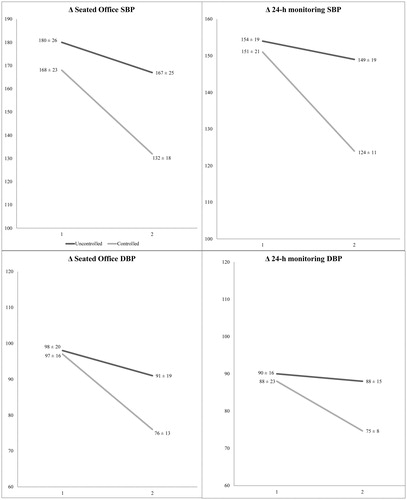
Table 2. Predictors of eventual blood pressure control at last follow-up in the expert centre.
Figure 3. Hypothetical model of the interactions between drug adherence, psychological profile and target organ damage in the pathogenesis of resistant hypertension.
Target organ damage, poor drug adherence and previous traumatic experiences/altered psychological profiles are the cornerstones of resistant hypertension, the “white elephant” in the field. They may be involved either separately or jointly. A few possible scenarios include: (i) poor drug adherence (2) may lead to TOD (1), which increases drug resistance even when drug adherence is afterwards improved; (ii) in hypertensive patients with increased arterial stiffness and/or TOD (1), reaching BP control may be difficult, inducing them to stop medications because of discouragement (2); (iii) altered psychological profiles (3) may be responsible for intentional (i.e. Münchausen syndrome) poor adherence (2), leading to an increased risk of TOD and finally of RHTN (1); (iv) or induce neuro-hormonal or inflammatory changes eventually leading to RHTN (1), irrespective of drug adherence.