Figures & data
Table 1. Clinical and cosmetic signs of prostaglandin-associated periorbitopathy syndrome (PAPS)
Figure 1. A case of DUES caused by treatment with benzalkonium chloride (BAK)-preserved tafluprost ophthalmic solution.
The most prominent feature of PAPS is the appearance of, or worsening of, DUES. This case shows a case of DUES caused by treatment with BAK-preserved tafluprost ophthalmic solution. This 59-year-old woman showed DUES OS 2 months after starting tafluprost ophthalmic solution (b; white arrow). (a–d) Time points: 0 months (starting point), 2, 4, and 6 months after starting tafluprost, respectively.Images provided by Sakata R. Figure reproduced with permission from Sakata et al. (Jpn J Ophthalmol. 2014 Mar;58(2):212–7. doi: 10.1007/s10384-013-0299-8.)Citation6; copyright 2014 Japanese Ophthalmological Society (within Japanese Journal of Ophthalmology).
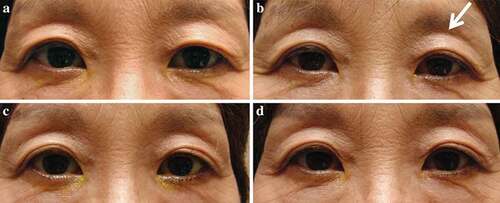
Figure 2. Notable signs of PAPS.
Notable clinical and cosmetic signs of PAPS include FLEB, DUES, upper eyelid ptosis, and orbital fat atrophy.(A; left) A 25-year-old female who had used bimatoprost for glaucoma in both eyes for 25 months. Conjunctival injection and signs of PAPS, including DUES, mild inferior scleral show, and mild dermatochalasis, were observed. (B; right) A 68-year-old male who had been using bimatoprost eye drops in both eyes for several years. Both eyes showed marked upper eyelid lipoatrophy (i.e. DUES).Informed consent has been obtained for both patients. Images provided by Chang PY (A; left) and Sakata R (B; right).

Figure 3. Mechanism of action and impact of PGAs on adipose changes in PAP.
FP2α: prostaglandin F2α receptor; LPL: lipoprotein lipase; MAPK: mitogen-activated protein kinase; P: phosphorylation;PGA: prostaglandin analog; PGF2α: prostaglandin F2α; PPARγ: peroxisome proliferator activated receptor gamma.Adapted from: Sarnoff et al. (2015).Citation11
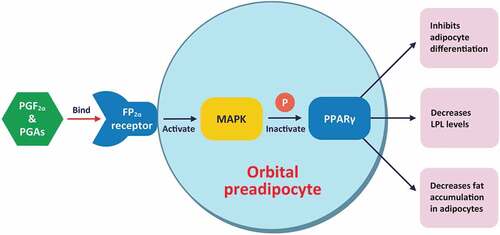
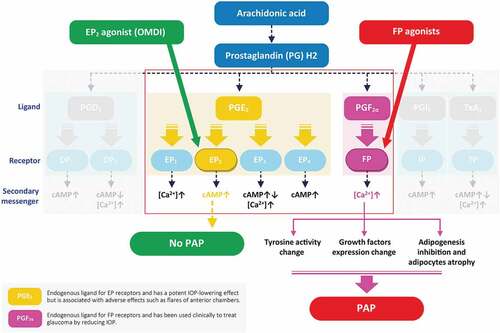
Figure 4. Receptor-based mechanism of action.
cAMP: cyclic adenosine monophosphate; DP1: PGD2 receptor 1; DP2: PGD2 receptor 2; EP: prostaglandin E receptor; FP: prostaglandin F receptor; IOP: intraocular pressure; IP: prostacyclin receptor; OMDI: omidenepag isopropyl; PAP: prostaglandin-associated periorbitopathy; PGD2: prostaglandin D2: PGE2: prostaglandin E2; PGI2: prostacyclin;PGF2α: prostaglandin F2α; TP: thromboxane A2 receptor; TxA2: thromboxane A2.Adapted from: Doucette et al. (2017)Citation25; Taketani et al. (2014)Citation27; Johnstone et al. (2002)Citation28; Mohan et al. (2012)Citation29; Dutkiewicz et al. (2000)Citation30; Fuwa et al. (2018).Citation31