Figures & data
Figure 1. Preoperative extraoral view reveals a prominent bulge coated with normal skin color and temperature. Postoperative photographs reveals a basically symmetrical facial profile (b) frontal view; d. right side view), and (c) normal mouth opening of 45 mm.

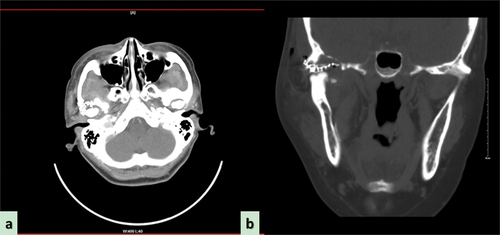
Figure 2. Preoperative computed tomography scan reveals the wormlike osteolysis of the right condylar head presenting with swelling, cloudy flocculent ground-glass opacity, relatively clear boundary, thin bone in the middle of the cranial fossa, low continuity, and involving the temporomandibular joint. (a) Computed tomography (CT) sagittal plane, (b) CT axial plane, (c) CT coronal plane. (d) Preoperative magnetic resonance imaging reveals the lesion exhibiting hypointensity, presenting as an oval soft tissue shadow on the sagittal T1-weighted image. (e) Heterogeneous hyperintensity on the axial T2-weighted image and (f) T1-enhanced weighted image in the coronal position shows ring enhancement.
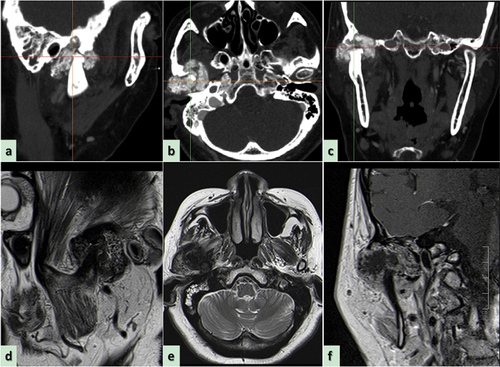
Figure 3. Morphological characteristics of preoperative biopsy using fine needle aspiration revealed through hematoxylin-eosin staining. (a) Abundant mucoid and loosely distributed spindle-shaped or stellate cells (black asterisk, original magnification × 100), and rich fibrous septal lobes in cartilage matrix (black arrow, original magnification × 100); (b) an atypical lesion of fibrous septal lobe containing circularly close-packed cells surrounding clear mucus and extracellular matrix (black triangle, original magnification × 200); (c) a large amount of mononuclear spindle-like stromal cells mixed with occasional multinucleated giant cells (black arrow, original magnification × 400).

Figure 4. Digital design and fabrication of simulation model for reconstructive surgery. (a,b) the close relationship between the tumor and blood vessels; (c) image registration technique and inverse design for restoring the anatomical shape of the destruted fossa [Citation8]; (d,e) 3D printing model displaying the exact location of the tumor and the nature of its relationship with the peripheral blood vessels, nerves, and other tissues; (f) placement of titanium mesh preoperatively.
![Figure 4. Digital design and fabrication of simulation model for reconstructive surgery. (a,b) the close relationship between the tumor and blood vessels; (c) image registration technique and inverse design for restoring the anatomical shape of the destruted fossa [Citation8]; (d,e) 3D printing model displaying the exact location of the tumor and the nature of its relationship with the peripheral blood vessels, nerves, and other tissues; (f) placement of titanium mesh preoperatively.](/cms/asset/273608fa-61be-4387-a2a1-80dfceafd0bb/ycra_a_2357988_f0004_oc.jpg)
Figure 5. Intra-operative photographs with high magnification.
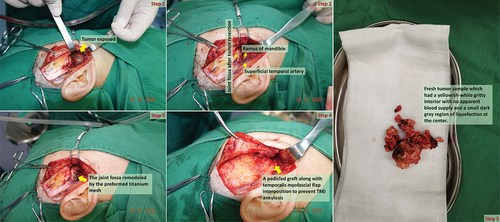
Figure 6. Photomicrograph of the tumor following hematoxylin-eosin staining and immunohistochemistry. (a) The cellular components are less prominent in cartilage matrix and mucoid (black triangle, original magnification × 200), but myofibroblastic-like spindle cell proliferation with loosely arranged myxoid stroma, minimal cellular atypia, and rare mitoses, along with storiform or fascicular pattern can be observed in the remaining areas; (b) a small amount of multinucleated giant cells (black arrow, original magnification × 400) admixed with plentiful mononuclear spindle cells surrounding clear mucus and cartilage matrix forming a pathologic lobular structure; (c) immunohistochemical staining is positive for S-100 in the chondrocytes (white asterisk, original magnification × 200) (d) but negative for Ki-67 in all kinds of cells (less than 1% positive).
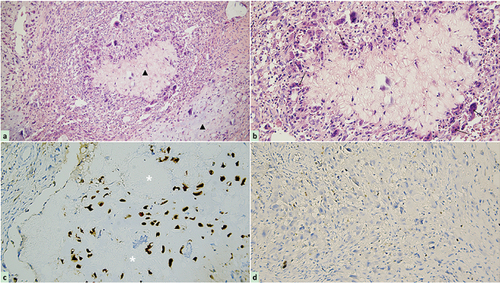
Figure 7. Computed tomography (CT) examination conducted 3 months postoperatively confirmed no signs of recurrence. (a) Axial plane; (b) coronal plane.